

Quick Summary: DHI and FUE are both modern follicular-unit hair transplant methods. The core difference is implantation: FUE creates recipient channels first and places grafts afterward, while DHI uses a Choi implanter pen to place follicles directly without pre-made channels.
For Canadian patients, the right choice depends on density goals, shaving preferences, visible downtime, donor quality, and CAD cost. This guide explains the decision clearly, without treating either method as universally “better.”
For Canadian patients researching Istanbul hair restoration, DHI vs FUE hair transplant is one of the most common technique questions. Both methods can produce natural results when the donor area, graft handling, angle control, and hairline planning are done properly. The difference is not whether one is “modern” and the other is outdated. The real difference is how the grafts are implanted.



At AKM Clinic, patients comparing DHI hair transplant at AKM Clinic with FUE are assessed through a practical lens: how much density is needed, how visible the recovery can be, whether shaving is acceptable, and how much precision is required around the frontal hairline. A patient from Toronto who works client-facing may value unshaven DHI more than a patient from Calgary who can take two weeks away from public work. Technique should follow anatomy and lifestyle.
This article is a decision tree, not a sales argument. It will help you understand where DHI and FUE overlap, where they differ, and which route may make more sense before you book a virtual consultation.
Table of Contents
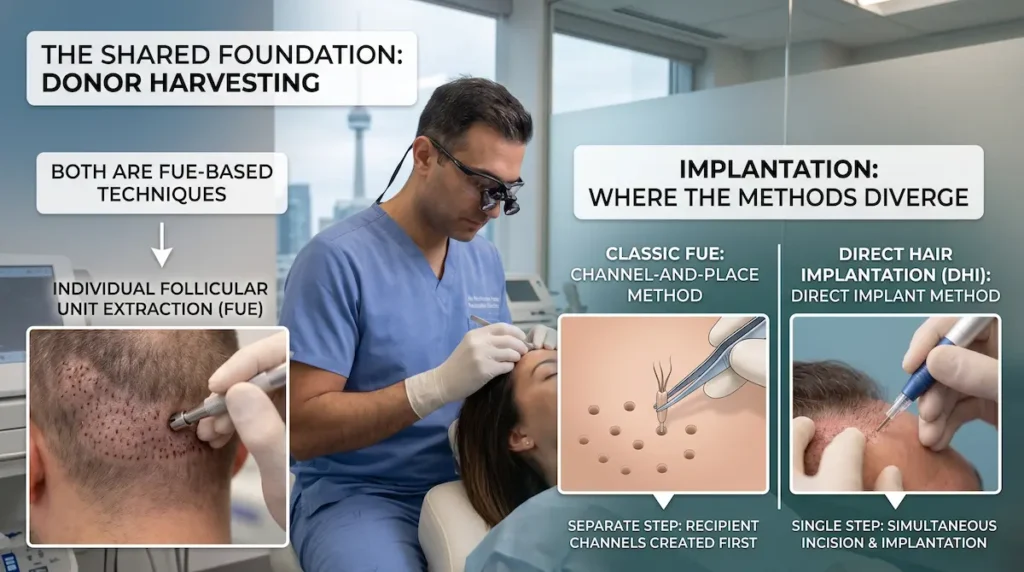
The Shared Foundation — Both Are FUE-Based
DHI and FUE are often presented as completely separate procedures, but that creates confusion. Both depend on extracting individual follicular units from a donor area, usually the back and sides of the scalp. The shared foundation matters because donor quality, surgical planning, and graft survival influence the result more than the label alone.
Follicular Unit Extraction Basics
Follicular unit extraction removes natural groupings of hair follicles one by one. These units may contain one, two, three, or occasionally four hairs. They are harvested from stable donor zones and then relocated to thinning or bald areas.
The International Society of Hair Restoration Surgery describes FUE as a method that removes individual follicular units from donor regions for transplantation into areas that need coverage. ISHRS patient guidance on FUE supports this basic definition. For Canadian context, the Canadian Dermatology Association’s alopecia and hair transplant resource explains that transplantation may be an option for some pattern baldness cases and involves moving follicles from healthy-growth areas to thinning or bald areas. For Canadian patients, the key point is simple: the extraction principle is similar in both DHI and FUE.
Where DHI and FUE Diverge
The main difference appears after grafts are extracted. In classic FUE, the surgeon or surgical team first creates tiny recipient channels in the scalp. The grafts are then inserted into those channels. This is why FUE is often called a channel-and-place method.
In DHI, the extracted grafts are loaded into a Choi implanter pen. The pen allows the clinician to control angle, direction, and depth as the follicle is implanted. There is no separate channel-opening step in the same way. That distinction is why DHI is often preferred for selected patients who need refined density in a smaller or more visible area.
Why “DHI vs FUE” Is Really an Implantation Comparison
Most online comparisons exaggerate the difference. The fairer way to frame the question is this: Do you need a channel-first implantation method or a direct-implantation method? That answer depends on your loss pattern, donor capacity, hair calibre, scalp laxity, and expectations.
“Technique selection should start with the patient’s hair loss pattern, not with marketing. A dense frontal hairline, a large crown, and an unshaven professional recovery each point to different priorities.”
Canadian Patient Note
Patients travelling from Vancouver, Montreal, Toronto, or Ottawa often compare technique by recovery visibility. That is reasonable. Still, visible downtime is only one factor. A good plan also protects donor supply for future hair loss, especially in younger male patients.
FUE — Channel-and-Place Method
FUE remains one of the most established modern hair transplant approaches. It is versatile, predictable, and suitable for many scalp patterns. For Canadian patients who need broad coverage, especially across the crown or mid-scalp, the channel-and-place method can be an efficient and cost-conscious option.
How Channels Are Created
In FUE, recipient sites are created before graft placement. The surgeon makes tiny channels that determine the direction, angle, and distribution of the transplanted hair. This planning step is critical. A well-made channel pattern can produce a soft, natural look. A poorly planned one can make even healthy grafts look artificial.
Patients comparing the FUE hair transplant technique should ask how the clinic plans recipient angles, how the hairline is marked, and who performs each step. The channel design should match the patient’s existing hair direction, not a generic template.
Graft Placement Step
After the channels are created, grafts are placed into them with fine instruments. The placement step must protect the follicle bulbs from crushing, drying, or bending. That is why technician skill and supervision matter.
In large sessions, FUE can move efficiently because the team can separate the channel-making and graft-placement steps. This can be useful for patients who need many grafts across a wider area. It may also offer strong value when the patient’s priority is coverage rather than ultra-dense packing in a small zone.
Strengths and Limitations
FUE is often a strong fit for larger areas. It can address the frontal zone, mid-scalp, crown, or a combination, depending on donor supply. It also has several technique variants, including micro FUE, manual FUE, motorized FUE, Bio-FUE, Ice FUE, and robotic FUE.
Its limitation is not quality. Its limitation is precision in certain high-density or unshaven situations. Because channels are created first, the surgeon must predict graft placement in advance. That can still work very well, but it may be less flexible than DHI in small, visible, density-focused zones.
DHI — The Choi Pen Method
DHI is best understood as a direct-implantation method. The grafts are still extracted individually, but the implantation stage changes. Instead of opening recipient channels first, the follicles are placed with a Choi implanter pen. This gives the clinical team detailed control over angle, depth, and direction during placement.
Direct Implantation with the Choi Pen
The Choi implanter pen holds the graft and places it directly into the scalp. This can reduce handling time and allows careful placement between existing hairs. For patients who still have native hair in the recipient zone, that level of control can be valuable.
This is also why DHI is frequently discussed for patients who want a more discreet procedure. The unshaven DHI option can help selected Canadian professionals return to work with less obvious visible disruption, especially when the transplant area is not extremely large.


Denser Packing Capability
DHI can be helpful when the target is density rather than broad surface coverage. Because grafts are implanted directly, the clinician can place follicles close together with careful angle control. This does not mean every patient should choose DHI. It means DHI can be useful in the right density problem.
Dense packing must still respect blood supply. A responsible clinic will not chase maximum density at any cost. Grafts need oxygen, spacing, and healthy tissue to survive. Canadian patients should be cautious with any clinic promising extreme density without discussing donor limits and scalp condition.
Strengths and Limitations
DHI is often strongest for frontal refinement, smaller high-visibility areas, unshaven cases, and patients who want precise direction control. It can be a strong choice for executives, teachers, healthcare workers, and public-facing professionals who cannot easily hide a shaved recipient area.
Its limitation is efficiency over very large areas. DHI can take more time and may cost more than standard FUE. For a patient with extensive crown loss, FUE may deliver better value. For a patient needing frontal density with minimal visible downtime, DHI may be the better match.
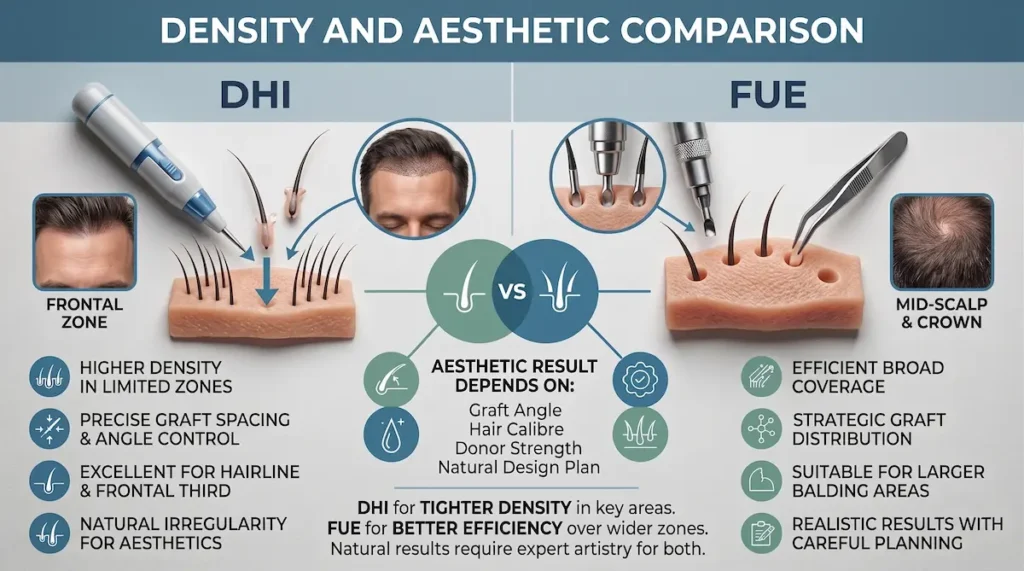
Density and Aesthetic Comparison
Density is where many DHI vs FUE comparisons become too simplistic. DHI can be useful for refined, high-density work in selected areas, while FUE can be more practical for broad coverage. The aesthetic result still depends on graft angle, hair calibre, donor strength, and a natural design plan.
Which Achieves Higher Density
DHI is often chosen when the patient needs density in a smaller, more visible zone. The Choi pen allows direct placement of grafts with careful control over angle and spacing. This can help in the frontal third, where density is immediately noticeable in photos, meetings, and daily interactions.
FUE can still create strong density. The difference is that FUE may be more efficient when the area is larger. A patient with diffuse thinning across the mid-scalp and crown may benefit more from strategic graft distribution than from dense packing in a limited area.
The honest answer is this: DHI may support tighter density in selected zones, while FUE may deliver better coverage efficiency. The surgeon should not promise density that the donor area cannot safely support.
Hairline Precision Differences
Hairline work is not just about placing grafts at the front. It requires irregularity, single-hair grafts, soft transition zones, and direction control. DHI can be helpful in this area because the implanter pen allows detailed placement at the moment of insertion.
FUE can also produce a natural hairline when recipient channels are planned carefully. The technique is not the only artistic variable. The surgeon must design a hairline that fits the patient’s age, forehead proportions, existing hair pattern, and future hair loss risk.
For the design principles behind both methods, see our guide to hairline design across both techniques. That separate article owns the deeper design discussion, while this comparison focuses on technique selection.
Whorl and Crown Coverage
Crown restoration is different from frontal work. The crown has a whorl pattern, which means grafts must follow a circular direction. It also consumes many grafts. A patient may need more donor supply for the crown than they first expect.
FUE is often practical for crown and mid-scalp coverage because it can distribute grafts across wider areas. DHI may still be used when direction control is especially important, but the time and cost-value balance must be considered. In many cases, the best plan is not “maximum density everywhere.” It is density where the eye notices it most.
Canadian Patient Note: Camera-Facing Work
Patients in Toronto, Vancouver, Montreal, and Ottawa often mention video calls, client meetings, and hybrid work schedules during consultation. If your frontal hairline is the visible concern, DHI may be worth discussing. If your priority is broader coverage under everyday lighting, FUE may be more practical.
Recovery and Healing Comparison
Recovery after DHI and FUE is similar in broad terms because both involve follicular extraction and scalp healing. The differences are usually about shaving, visible signs, recipient-area trauma, and how quickly a patient feels comfortable returning to professional life. The first two weeks matter most for appearance and graft protection.
Healing Speed Differences
DHI is sometimes described as faster healing because there is no separate channel-opening step. That can be true in selected cases, especially in smaller zones. Still, the patient should not assume DHI eliminates swelling, redness, scabbing, or shock shedding. It does not.
FUE healing is well understood and predictable when aftercare is followed closely. The donor area usually heals quickly, while the recipient area passes through redness, scabbing, and early shedding. The practical difference is often visibility, not medical recovery.
AKM Clinic’s hair team gives patients clear post-op instructions before they return to Canada. This matters because the most delicate recovery decisions happen after leaving Istanbul: washing, sun exposure, hat use, and avoiding friction.
Shaving Requirements: DHI Unshaven Option
Shaving is one of the biggest lifestyle differences between DHI and FUE. Standard FUE commonly requires shaving the donor and recipient areas so the team can extract, plan channels, and place grafts efficiently. Many patients accept this easily.
DHI can be performed as an unshaven option in selected cases. This is not a universal guarantee. It depends on hair length, density, the size of the recipient zone, and whether the team can work safely between existing hairs.

Canadian Patient Note: Unshaven DHI for Visible Downtime
Unshaven DHI can appeal to Canadian professionals who cannot take visible downtime. A lawyer in Toronto, a physician in Vancouver, or a teacher in Montreal may care less about the technical label and more about returning to work without an obvious shaved scalp. Candidacy must still be confirmed by photo review and consultation.
Growth Timeline Differences
DHI and FUE follow the same biological growth pattern. Transplanted hairs commonly shed in the early phase, then enter a resting period before new growth begins. Patients should not judge either technique too early.
Dense-packing cases, including many DHI plans, may take longer to look fully mature because fine early growth needs time to thicken. FUE results also mature gradually. The final comparison usually belongs at the 12- to 18-month mark, not at month three.
For the recovery arc after the grafts are placed, see our dedicated guide to growth timeline differences between techniques. This article stays focused on choosing the method before surgery.
Cost and Candidacy in CAD
Cost matters, but it should not be the first filter. The correct method is the one that fits your anatomy, donor capacity, desired density, and recovery limits. Once those clinical priorities are clear, CAD pricing helps compare value honestly.
DHI Pricing Tiers
AKM Clinic lists DHI techniques in the Treatment Techniques cost reference. Standard DHI, Mega Session DHI, and Unshaven DHI are all listed at the same CAD price tier. Robotic DHI is listed separately at a higher tier because it uses robotic precision support.
For exact technique-specific details, review DHI pricing in CAD. DHI pricing should be interpreted through candidacy: a patient choosing unshaven DHI for discretion may find the value very different from a patient who does not mind shaving.
FUE Pricing Tiers
FUE has more technique variants. Micro FUE, Motorized FUE, Ice FUE, Manual FUE, Bio-FUE, and Robotic FUE each serve different planning needs. Most patients do not need the most expensive variant. They need the variant that protects graft survival and matches the transplant area.
Patients comparing FUE can review FUE pricing in CAD before the virtual consultation. Pricing helps with planning, but final technique selection should come after donor assessment and hair loss pattern review.
Decision Tree — Matching Technique to Patient
The decision tree below gives a practical starting point. It does not replace consultation. It helps you understand which questions the surgeon is trying to answer when comparing DHI and FUE.
| Decision Factor | DHI | FUE |
|---|---|---|
| Implantation method | Direct placement using a Choi implanter pen | Recipient channels created first, then grafts placed |
| Best fit | Frontal density, refined zones, unshaven candidates | Broad coverage, crown work, larger surface areas |
| Density priority | Often stronger for selected dense-packing needs | Strong when planned across wider areas |
| Shaving | Unshaven option possible for selected patients | Shaving is commonly required for efficient planning |
| Recovery visibility | Often less visibly disruptive in unshaven cases | More visible early recovery if shaved recipient area is required |
| AKM CAD pricing | Standard DHI, Mega Session DHI, and Unshaven DHI: CAD $3,400; Robotic DHI: CAD $7,500 | Micro FUE, Motorized FUE, and Ice FUE: CAD $3,000; Manual FUE: CAD $3,850; Bio-FUE: CAD $3,150; Robotic FUE: CAD $7,500 |
The safest question is not “Which method is better?” It is “Which method solves my specific problem with the least donor waste?” Canadian patients should also confirm that the quote is fixed and clear before arranging flights. For pricing model details, see our fixed-price evaluation for either technique.
Canadian Patient Note: Cost-Value Decision
FUE may offer excellent value for broad restoration. DHI may offer stronger value when visible downtime, unshaven recovery, or frontal density is the main concern. The lower price is not always the better value. The better value is the method that avoids revision, protects donor supply, and fits your work schedule.
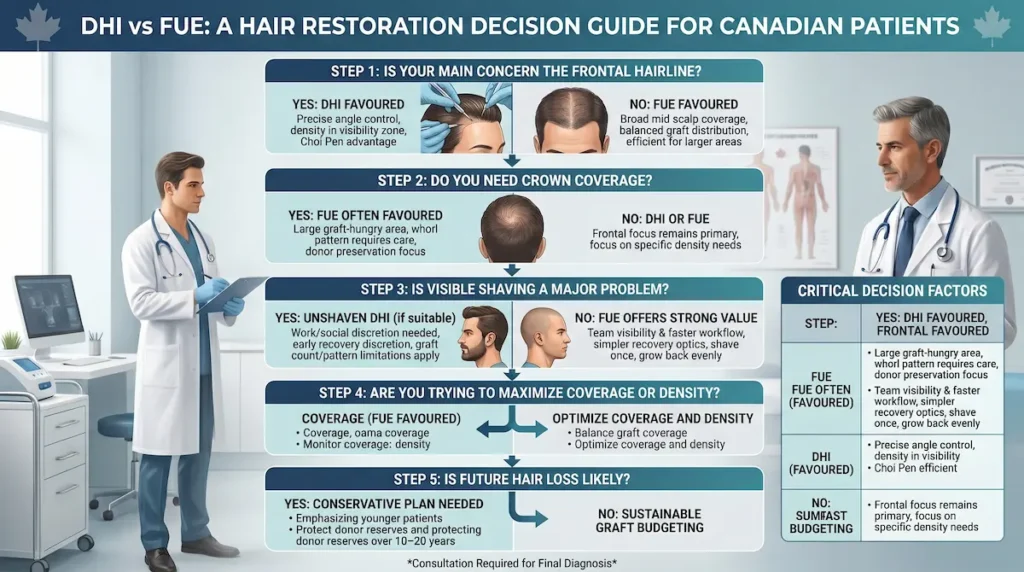
DHI vs FUE Decision Tree for Canadian Patients
The best technique is usually clear once the right clinical questions are asked. This decision tree turns the DHI vs FUE choice into a practical sequence: visibility, density, area size, donor supply, and budget. Use it as a pre-consultation guide, not as a final diagnosis.
Step 1: Is Your Main Concern the Frontal Hairline?
If your main concern is the frontal hairline, DHI may be worth prioritizing. The Choi pen can help the team place grafts with precise angle and direction control in a highly visible area. This is especially relevant if the goal is density along the first centimetres of the hairline.
If your concern is a broad area behind the hairline, FUE may be more efficient. Many patients need balanced distribution across the frontal third and mid-scalp rather than maximum density in one narrow zone. Coverage strategy matters.
Step 2: Do You Need Crown Coverage?
Crown work often favours FUE because the area can be large and graft-hungry. The circular whorl pattern also requires careful distribution. A surgeon may reserve stronger grafts for the front and use a conservative crown plan to preserve donor supply.
DHI can still be used in crown cases, but it is not always the most efficient choice. If a clinic recommends DHI for every crown patient, ask why. The answer should refer to your specific anatomy, not a blanket preference.
Step 3: Is Visible Shaving a Major Problem?
If visible shaving would create work or social difficulty, ask whether unshaven DHI is realistic. This can be helpful for patients who need discretion during early recovery. It is not appropriate for every graft count or loss pattern.
If shaving is acceptable, FUE may offer strong value. A shaved approach can give the team clearer visibility, faster workflow, and easier placement across larger areas. Many patients prefer the simpler recovery optics of shaving once and letting everything grow back evenly.
Step 4: Are You Trying to Maximize Coverage or Density?
Coverage and density are not the same. Coverage spreads grafts across a wider area. Density concentrates grafts in a smaller zone. Patients often want both, but donor supply sets limits.
If you want density in a specific frontal zone, DHI may be favoured. If you need a larger restoration, FUE may create a better overall result. A natural transplant usually comes from strategic compromise, not from placing every graft in the first area the patient notices.
Step 5: Is Future Hair Loss Likely?
Younger patients, especially those under 35, need a conservative plan. A low, dense hairline can look appealing today and become a problem later if surrounding hair continues to thin. Technique selection must account for the future.
DHI and FUE both use finite donor hair. Neither creates new follicles. A good plan protects donor reserves for future procedures if hair loss progresses. Canadian patients should ask how the chosen method preserves options over the next 10 to 20 years.
| Your Priority | Technique Often Favoured | Why |
|---|---|---|
| Frontal hairline density | DHI | Direct implantation can support detailed angle and density control. |
| Large mid-scalp or crown coverage | FUE | Channel-and-place workflow can be efficient for wider restoration areas. |
| Unshaven or discreet recovery | DHI, if clinically suitable | Unshaven DHI may reduce visible downtime for selected patients. |
| Cost-conscious broad restoration | FUE | Several FUE options sit at a lower CAD tier than DHI. |
| Future donor preservation | Depends on plan, not label | Both techniques require conservative graft budgeting. |
How AKM Clinic Evaluates DHI vs FUE Candidacy?
Technique selection at AKM Clinic begins with diagnosis. The consultation looks at donor density, hair calibre, loss pattern, age, hairline goals, and visibility concerns. This prevents the common mistake of choosing a procedure name before the scalp has been properly assessed.
Photo Review and Donor Assessment
The first step is usually photo-based review. Clear photos of the frontal hairline, temples, crown, donor area, and side profile help the team estimate the pattern of loss. This is especially important for international patients who are planning from Canada.
Donor strength affects every decision. Thick donor hair can create more visual coverage with fewer grafts. Fine-calibre hair may require a more careful density plan. DHI cannot overcome poor donor supply, and FUE cannot make unlimited coverage possible.
Density Planning and Hairline Approval
Before surgery, the hairline should be drawn and approved. The patient should understand why the proposed height, recession pattern, and temple transition have been chosen. A natural result is planned before any graft is placed.
This is where DHI may become attractive for frontal work. It allows detailed implantation in a visible zone. FUE may still be recommended if the patient needs broader coverage or if the density goal is better served by a channel-first plan.
Technique Recommendation and Patient Input
A good consultation does not force a technique. It explains the trade-offs. The patient’s work schedule, tolerance for shaving, desired density, and CAD budget all matter. The final recommendation should make clinical sense and practical sense.
AKM Clinic’s broader hair restoration approach also includes Low-Level Laser Therapy for hair restoration support. The clinic uses 424 medical-grade semiconductor laser diodes at 650 nm to support scalp microcirculation and follicle health as part of its technology infrastructure.
Frequently Asked Questions: DHI vs FUE Hair Transplant
These questions address the concerns Canadian patients most often raise before choosing between DHI and FUE. They are meant to clarify the decision, not replace a consultation based on your photos and donor assessment.
Is DHI Better Than FUE?
DHI is not automatically better than FUE. It may be better for selected patients who need refined frontal density, careful direction control, or an unshaven option. FUE may be better for patients who need wider coverage, especially across the mid-scalp or crown.
Which Is More Expensive at AKM in CAD?
Standard DHI, Mega Session DHI, and Unshaven DHI are listed at CAD $3,400. Several FUE options, including Micro FUE, Motorized FUE, and Ice FUE, are listed at CAD $3,000. Manual FUE is listed at CAD $3,850, while robotic options for both methods are listed at CAD $7,500.
Does DHI Require Shaving?
DHI can sometimes be performed unshaven, but not always. Unshaven DHI depends on the transplant area, hair length, graft count, and whether the team can safely work between existing hairs. Patients should confirm this during consultation rather than assuming they qualify.
Which Gives Higher Density?
DHI can support high-density placement in selected areas, especially the frontal hairline. FUE can also produce strong density when planned well. The better question is where density matters most and how many grafts your donor area can safely provide.
Which Has a Faster Recovery?
Recovery is broadly similar because both methods involve follicular extraction and scalp healing. DHI may have less visible disruption in selected unshaven cases. FUE may look more obvious early if the recipient area is shaved, but medical recovery can still be straightforward.
Can I Have a Combination of Both?
Yes, some patients may benefit from a combined approach. A surgeon might use DHI for the frontal hairline and FUE principles for broader coverage elsewhere. The combination should be chosen for clinical reasons, not because it sounds more advanced.
Which Is Right for My Hair Loss Pattern?
DHI often suits smaller, visible, density-focused zones. FUE often suits larger areas and crown work. Your age, donor quality, future hair loss risk, and willingness to shave will shape the final recommendation.
Choosing between DHI and FUE should not start with a technique preference. It should start with a clear diagnosis: where you are thinning, how strong your donor area is, how much visible downtime you can accept, and what kind of density will look natural over time.
AKM Clinic evaluates these factors through photo review and virtual consultation before recommending a method. Some Canadian patients are better matched to DHI because they need frontal precision or unshaven discretion. Others are better matched to FUE because they need broader coverage and strong cost-value.
To determine your ideal technique, request a virtual consultation and ask the team to compare DHI and FUE against your actual hair loss pattern, not against a generic online checklist.
Medical Disclaimer: This page is provided for general educational purposes only and does not replace an in-person medical consultation, diagnosis, or personalized treatment plan. All surgery carries risks, and outcomes vary between individuals. Suitability for a hair transplant, procedure selection, and anesthesia choice can only be determined after a full clinical assessment by a qualified surgeon. Always follow your clinician’s instructions and seek urgent medical attention if you develop concerning symptoms during recovery.










