









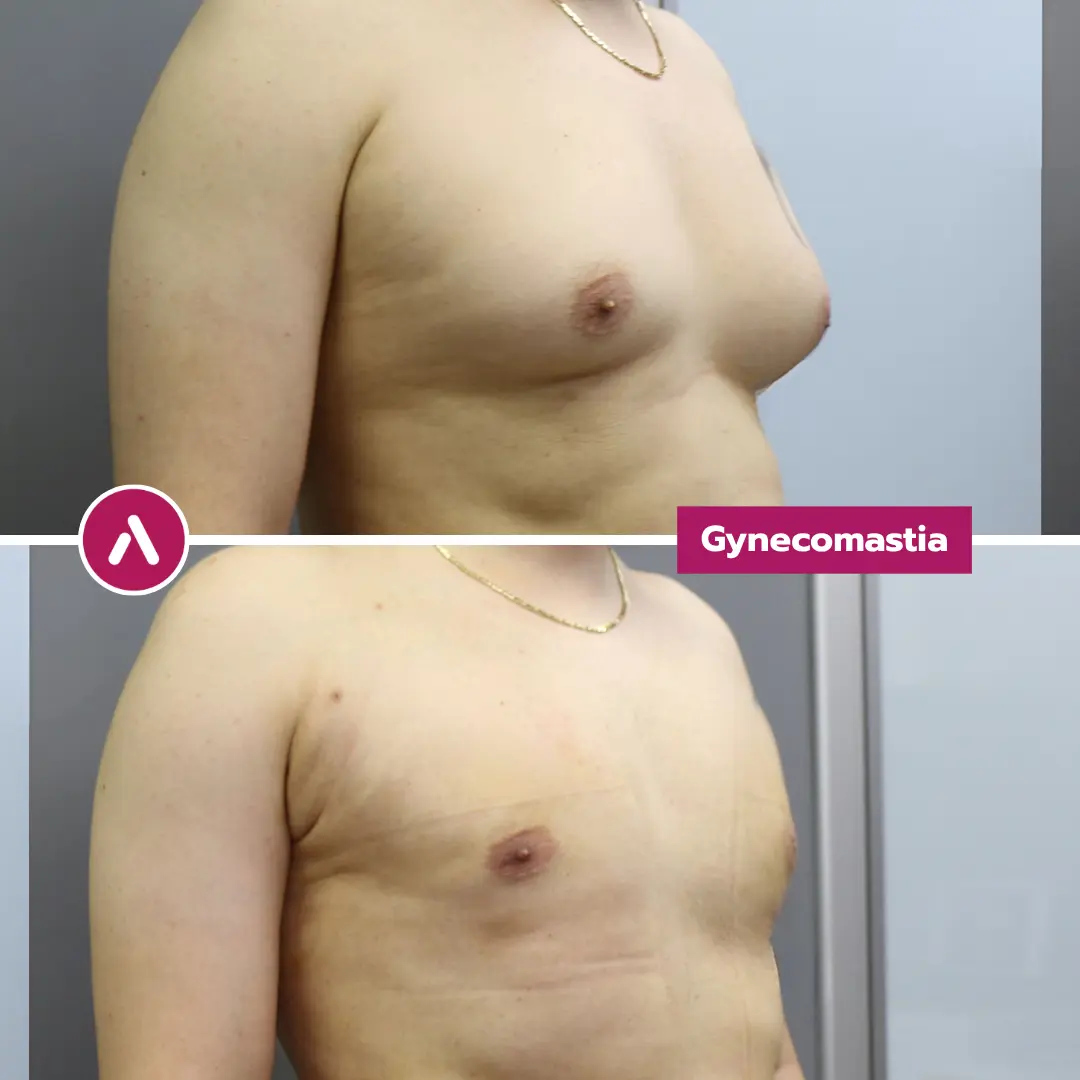
For many men, chest fullness isn’t ‘just fat’. Gynaecomastia Surgery reduces male breast enlargement by treating the true cause—fat, glandular tissue, or both—so the chest looks naturally flat in clothing and at the gym. We assess pseudogynecomastia vs true gynaecomastia, grade severity, and plan scars to sit discreetly around the areola.
Designed for UK patients, our pathway focuses on safety, comfort, and predictable recovery. Suitable candidates may choose awake/twilight sedation with local anaesthetic, structured compression and follow-up, and travel-aware aftercare. If you want a medically grounded plan—rather than a one-size-fits-all ‘lipo’ solution—request a clinical assessment and clear practical next steps.
Table of Contents
What is Gynaecomastia Surgery?
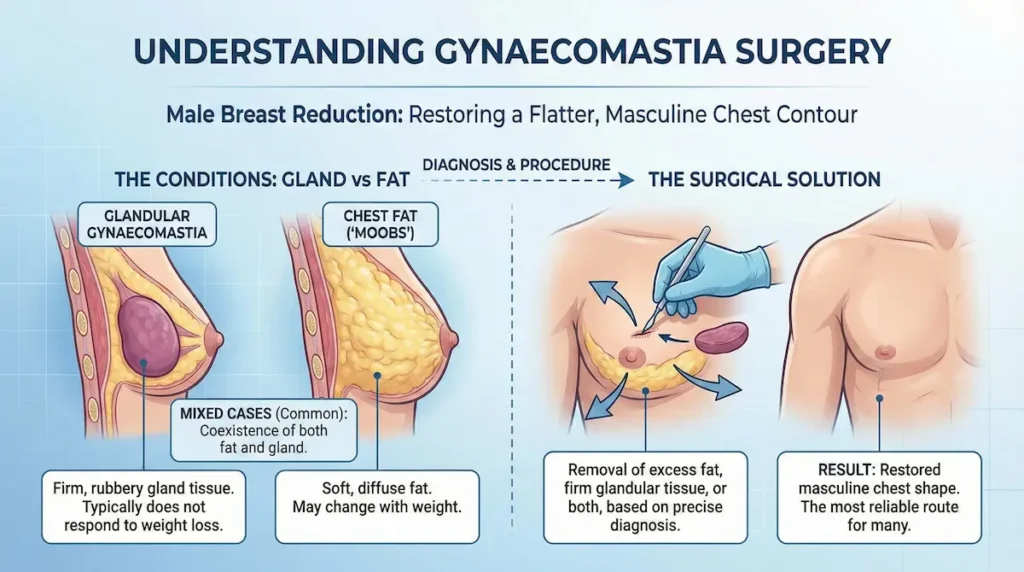
Gynaecomastia Surgery is a procedure that reduces male breast enlargement by removing excess fat, firm glandular tissue, or both. It aims to restore a flatter, more masculine chest contour. For many men, it is the most reliable route when exercise and weight loss do not change the chest shape. The plan is always based on what is causing the fullness.
In practical terms, this is often described as male breast reduction. The key point is diagnosis: some chests are mostly fat, while others contain a dense gland behind the nipple-areola complex. Treating the wrong problem leads to disappointment, so we start with anatomy and a clear surgical rationale.
“Man boobs” (moobs) vs true gynaecomastia (gland vs fat)
Many UK patients begin by searching for man boobs or moobs. Those terms describe the appearance, not the cause. The cause matters, because fat responds to weight change while glandular tissue typically does not.
- Chest fat: soft, diffuse fullness that often changes with weight.
- Glandular gynaecomastia: a firmer, rubbery disc-like tissue, commonly felt under the areola.
- Mixed cases: very common; fat and gland can coexist.
In your consultation, we focus on the “why” before the “how”. That is how we keep the plan precise and the result natural.
Gynaecomastia vs pseudogynecomastia (why the difference matters)
Pseudogynecomastia refers to chest enlargement that is primarily fatty tissue rather than true gland growth. It can look identical in clothing. It behaves differently once we treat it.
If the issue is mostly fat, contouring is about smooth transitions across the chest wall. If the issue includes a true gland, the aim is a flatter subareolar profile, while protecting the nipple-areola contour from looking “stuck on” or indented.
This is where an “expert patient” mindset helps. Instead of asking “Do I need lipo?”, ask “Is there a gland, fat, or both?” That one question usually clarifies the pathway.
When does surgery become the “definitive” option?
Non-surgical steps can help in select situations, but they have limits. If your chest shape is driven by firm gland tissue, there is rarely a meaningful change from training alone.
- You have persistent fullness despite stable weight and consistent exercise.
- You can feel a firm subareolar lump that does not shift with weight change.
- The appearance affects clothing choices, posture, or confidence in social settings.
Our guiding principle is simple: achieve a subtle, authentic result that looks like your chest always belonged to you.
Symptoms, Assessment, and Grading: How Do We Measure Severity?
Before any technique is discussed, we assess the pattern of fullness and how the skin behaves. That assessment answers three practical questions: what tissue is present, how much there is, and whether the skin will re-drape after reduction. A good plan is not just “removal”; it is controlled contouring with long-term stability in mind.
For UK patients comparing NHS pathways vs private options, this step-by-step classification is often the missing piece. When you understand your grade, you can judge whether a proposed plan makes sense. You also avoid being oversold a “one size fits all” approach.
The “pinch test” and what it can (and cannot) tell you
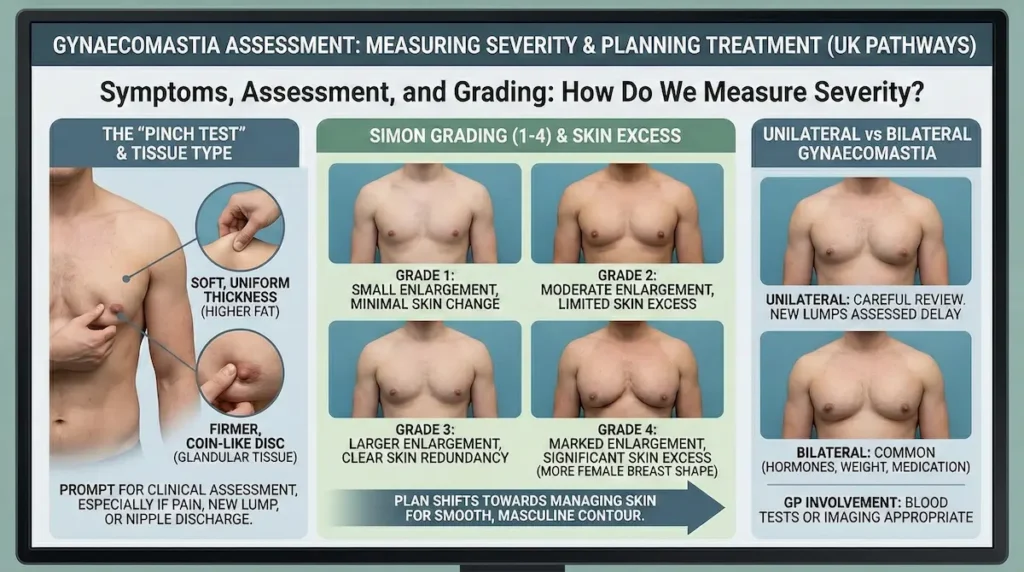
The gynaecomastia pinch test is a simple self-check that gives clues about tissue type. Gently pinch the tissue near the areola and then higher on the chest.
- Soft, uniform thickness across the chest often suggests a higher fat component.
- A firmer, coin-like disc directly under the areola suggests glandular tissue.
- Asymmetry is common; each side may need a different emphasis.
It is not a diagnosis. It is a prompt for a proper clinical assessment, especially if there is pain, a new lump, or nipple discharge.
Grades 1–4 (Simon grading): what changes as the grade increases?
Simon grading gynaecomastia is a practical way to describe size and skin excess. It helps set expectations about scars, tightening, and how “flat” the chest can look early on.
- Grade 1: small enlargement, minimal skin change.
- Grade 2: moderate enlargement, limited skin excess.
- Grade 3: larger enlargement with clear skin redundancy.
- Grade 4: marked enlargement with significant skin excess, more like a female breast shape.
As grades rise, the plan may shift from simple reduction towards managing skin and achieving a smooth, masculine contour line.
Unilateral vs bilateral gynaecomastia: when should you investigate further?
Bilateral gynaecomastia is common and often linked to hormones, weight changes, or medication history. Unilateral gynaecomastia can still be benign, but it deserves a more careful review.
- New or rapidly changing lumps should be assessed without delay.
- Persistent tenderness may relate to active tissue changes or medication triggers.
- Your GP may be part of the pathway if blood tests or imaging are appropriate.
Our role is to be clinically straightforward. If surgery is appropriate, we plan it carefully. If something needs investigating first, we say so.
Benefits of Gynaecomastia: What Changes After Treatment?
The main goal is straightforward: a flatter, more masculine chest that looks natural in motion and in clothing. Most patients are not trying to look “enhanced” — they want the chest to stop being the first thing they notice in the mirror.
The best outcomes come from two things working together: accurate tissue diagnosis (fat vs gland vs both) and an aesthetic plan that respects your anatomy (areola position, chest width, and skin quality).
Physical goal: a flatter, natural male chest contour
A successful result is not just “smaller”; it is smoother. That means a natural transition from the upper chest into the lower chest, without lumps, ridges, or an overly hollowed look under the nipple.
- Reduction of forward projection (less “puffy” appearance)
- Improved chest line in fitted clothing
- Better definition when training — without the chest still looking rounded
Early swelling can disguise the final contour, so judging the result too soon is a common mistake. We set timelines clearly so expectations stay realistic.
Clothing, posture, and the psychology of confidence
Many men adapt in small ways for years: layering clothes, avoiding light fabrics, rounding the shoulders, or skipping swimming and holidays. These behaviours are often as significant as the physical appearance itself.
When the chest sits flatter, patients commonly report they:
- choose clothes for style, not camouflage
- stand more upright without “guarding” the chest
- feel more comfortable in gyms, changing rooms, and social settings
Fitness and “pecs vs chest fat”: why training may finally show
A frequent UK search is man boobs vs pecs. In reality, pectoral muscle and soft tissue can exist together. If gland or fat dominates the visible shape, building muscle may not translate into the chest look you want.
After reduction, training can become more “rewarding” visually because:
- the chest contour reflects muscle structure more clearly
- definition around the upper chest becomes easier to appreciate
- your posture often improves, which changes how the chest is displayed
Think of the aim as refinement, not reinvention: a chest that looks like yours — just free from unwanted fullness.
Am I a Suitable Candidate?
Suitability is not only about how your chest looks today. It is about safety, predictable healing, and whether the plan matches your tissue type and lifestyle. A responsible clinic will tell you when to proceed and when to pause.
Key criteria: stable weight, realistic expectations, and a clear diagnosis
The most reliable candidates typically have a stable weight and understand that the chest will continue to mature for months after treatment. We also confirm whether you have primarily fat, gland, or a mixed case — because that determines the technique and the likelihood of a “definitive” result.
- Stable weight and sustainable routine
- Clear motivation (for you, not for external pressure)
- Comfort with a structured recovery period (compression garment, activity limits)
Age and timing: pubertal gynaecomastia vs adult presentation
Pubertal gynaecomastia can improve naturally in some teenagers as hormones stabilise. In adults, persistent enlargement is more likely to remain unless treated. Timing decisions should be individual and medically sensible.
In practical terms, if your chest shape has been stable for a long period and does not respond to lifestyle changes, a surgical solution becomes more reasonable to consider.
Who should delay or avoid treatment (for now)?
Sometimes the best decision is not “no”, but “not yet”. We may advise postponing if there is a factor that increases risk or reduces predictability.
- Uncontrolled medical conditions or a need for further investigation of new symptoms
- Active nicotine use (slower healing and higher complication risk)
- Unstable weight (ongoing significant loss or gain)
- Medication-related triggers that need medical review first
If something needs assessment before proceeding, we will be direct about it. The goal is the safest route to the best long-term outcome.
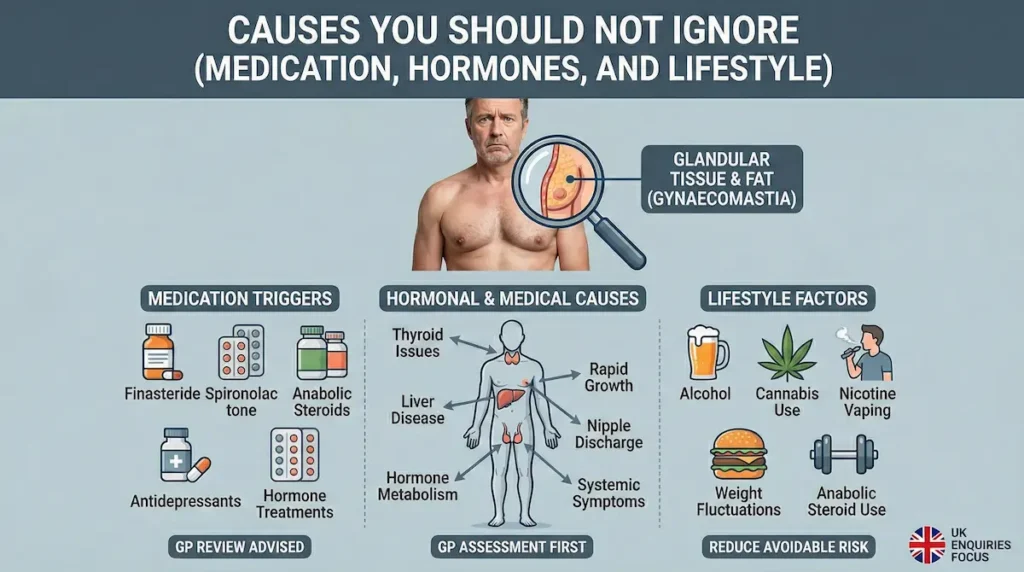
Causes You Should Not Ignore (medication, hormones, and lifestyle)
We see a pattern in UK enquiries. Many men assume their chest shape is “just fat”, then discover a firm gland is the real driver. The next question is sensible: why did it happen? Understanding triggers matters for two reasons. It helps you rule out medical issues that need a GP review, and it reduces the chance of recurrence if a preventable cause is still active.
We also hear the same search intent: moobs reduction without surgery. For purely fatty cases, lifestyle changes can make a difference. When true glandular tissue is present, non-surgical options tend to plateau. That is not pessimism. It is anatomy.
Medication triggers: what to check before you plan surgery
Some prescriptions and supplements can shift hormone balance or receptor activity and contribute to breast tissue changes. If you are taking any long-term medication, we review it as part of your clinical history. We do not ask you to stop anything abruptly. We help you approach it safely, often with input from your GP or prescribing clinician.
- Finasteride gynaecomastia: some men notice tenderness or tissue changes after starting or changing dose.
- Spironolactone side effects: can include breast tenderness or enlargement in susceptible patients.
- Other common culprits include certain antidepressants, anabolic steroids, and hormone-related treatments.
Hormonal and medical causes: when a GP assessment is the smart move
Most cases are benign. Still, we treat new symptoms with respect. If you have a new lump, rapid growth, nipple discharge, or significant pain, a GP assessment is the right first step. The same goes for clear systemic symptoms (fatigue, unexplained weight loss, testicular changes).
We may also discuss contributing conditions that can alter hormone metabolism, such as liver disease or thyroid issues. Surgery can still be an option later. The order matters.
Alcohol, cannabis, and lifestyle factors (the conversation most clinics avoid)
Some men specifically ask about cannabis induced gynaecomastia (or marijuana). The honest answer is that bodies vary and research is not always definitive on individual causation. What we can do is practical: we take a full history, we look for patterns, and we reduce avoidable risk.
- Keep weight stable before planning treatment.
- Avoid anabolic steroid use; it is a common and preventable trigger.
- If you are smoking or vaping nicotine, stopping improves healing and lowers complication risk.
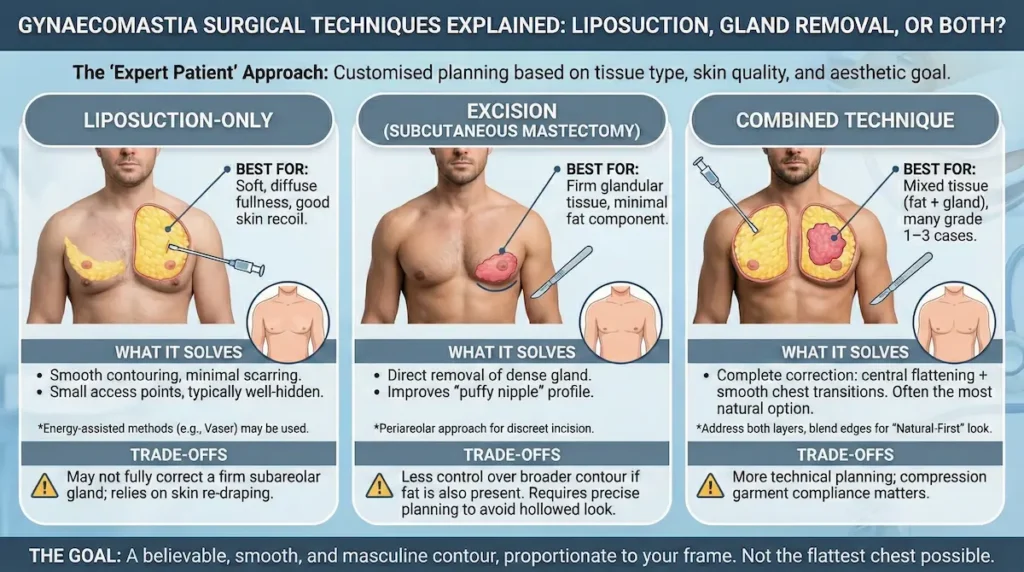
Gynaecomastia Surgical Techniques Explained: Liposuction, Gland Removal, or Both?
Here is where “expert patient” logic pays off. There is no single best technique for everyone. The right approach depends on tissue type, grade, skin quality, and your aesthetic goal. We plan the chest like a contour map, not a single “take it out” action. Small differences in judgement can change the final look.
In many cases, the key decision is whether you need gland removal in addition to fat reduction. Liposuction shapes. Excision solves a dense subareolar mound. A combined approach often delivers the most predictable male chest contour.
Liposuction-only: when it works well
Liposuction can be an excellent choice when the fullness is largely fatty and the skin has good recoil. It allows smooth contouring across the chest wall with minimal scarring. In selected cases, we may use energy-assisted methods (such as Vaser-assisted liposuction) when appropriate for tissue quality and definition.
- Best suited to soft, diffuse fullness
- Small access points, typically well-hidden
- Relies on skin re-draping for the final look
Excision (subcutaneous mastectomy): when the gland is the problem
If there is a firm gland under the areola, liposuction alone may leave a “puffy nipple” look behind. In these cases, we use direct excision to remove glandular tissue. The incision is often planned around the areola border (a periareolar approach) to keep it discreet.
- Targets the dense tissue that does not respond to diet or training
- Helps flatten the subareolar profile
- Requires precise contour planning to avoid a hollowed look
Combined technique: why it is often the most natural option
Many men have mixed tissue. Fat sits broadly across the chest while gland sits centrally. Combining liposuction and excision lets us address both layers, then blend the edges for a smooth transition. This is where our “Natural-First” mindset shows up in the details.
| Technique | Best for | What it solves | Trade-offs to understand | Typical scar pattern |
|---|---|---|---|---|
| Liposuction-only | Mainly fatty chest fullness, good skin recoil | Contour shaping and reduction of diffuse volume | May not fully correct a firm subareolar gland; relies on skin tightening | Very small access points, usually well-hidden |
| Excision-only (gland) | Firm glandular tissue with minimal fat component | Direct removal of dense gland; improves “puffy nipple” profile | Less control over broader contour if fat is also present | Often a discreet periareolar scar |
| Combined (lipo + excision) | Mixed tissue (fat + gland), many grade 1–3 cases | Complete correction: central flattening + smooth chest transitions | More technical planning; compression garment compliance matters | Periareolar scar + small lipo entry points |
Our aim is not the flattest chest possible. It is the most believable one — smooth, masculine, and proportionate to your frame.
Gynaecomastia Scars and Aesthetic Planning (keeping the result natural)
Most UK patients worry about scars as much as the chest shape itself. That is reasonable. A good plan balances two priorities: removing the right tissue and placing incisions where they heal discreetly. In gynaecomastia work, subtlety is the point — the best scar is the one you stop thinking about.
Where are the scars typically placed?
When gland excision is required, a common approach is a periareolar incision (along the edge of the areola). This border naturally camouflages fine lines as the scar matures. When liposuction is part of the plan, tiny access points may be used in hidden creases.
- Periareolar scars usually blend into the colour change between areola and surrounding skin.
- Small liposuction entry points are typically placed to be hard to notice when standing.
- Scar visibility depends on skin type, healing biology, and aftercare compliance.
Scar maturation: what timeline should you expect?
Scars do not “finish” in a few weeks. They mature over months. Early redness and firmness are normal phases of healing, not signs something has gone wrong.
- Weeks 1–6: incision lines may look pink, feel firm, and be slightly raised.
- Months 2–6: scars typically soften and begin to fade; swelling reduces and contour becomes clearer.
- Months 6–12: the scar often reaches its most settled appearance.
We guide you through the steps that support calm healing: protecting the area, avoiding unnecessary friction, and following garment guidance.
Avoiding the “overdone” look: why contour matters more than removal
Some men fear a “crater deformity” under the nipple (an overly hollowed appearance). This is preventable with careful technique and realistic goals. The chest should look flat but not “scooped out”.
That is why we plan:
- how much to remove centrally vs peripherally
- how to blend edges so transitions are smooth
- how to preserve a natural male chest thickness under the areola
In male chest contouring, precision is everything: enough reduction to look naturally flat, not so much that it looks artificial.
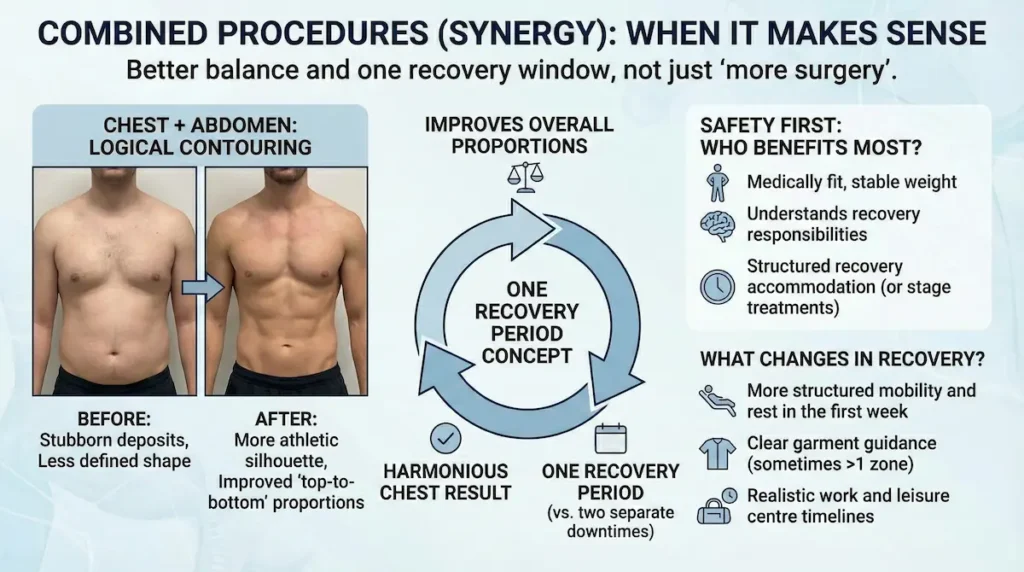
Combined Procedures (Synergy): When It Makes Sense
Some patients ask if they should treat only the chest or also address surrounding areas. Combining procedures can be sensible when it improves overall proportions and does not compromise safety. The point is not “more surgery”. It is better balance and one recovery window.
Chest + abdomen: when combined contouring is logical
If your overall goal is a more athletic silhouette, chest correction can pair well with abdominal or flank contouring. This is especially relevant when weight loss has improved general shape but left stubborn deposits. Depending on your anatomy and goals, this may involve liposuction for contour refinement, abdominal etching for enhanced definition, or a tummy tuck when skin excess needs surgical tightening.
- Improves “top-to-bottom” proportions
- Can make the chest result look more harmonious
- One recovery period instead of two separate downtimes
Adding other areas: when an arm lift can complement chest work
In selected patients—particularly after significant weight loss—upper arm skin laxity can affect overall silhouette. In these cases, an arm lift may be considered alongside chest correction to create a more consistent, athletic upper-body contour, provided safety and recovery planning remain appropriate.
Safety first: who benefits most from combining procedures?
Combination planning is typically best for patients who are medically fit, have stable weight, and understand recovery responsibilities. If your schedule or lifestyle cannot accommodate a structured recovery, it may be better to stage treatments.
What changes in recovery when procedures are combined?
Recovery planning becomes more important, not more complicated. You may need:
- more structured mobility and rest in the first week
- clear garment guidance (sometimes more than one garment zone)
- realistic work and gym timelines
We keep the plan practical for UK patients, including return-to-work planning and travel logistics. patients, including return-to-work planning and travel logistics.
Anaesthesia: Why Many Patients Prefer Awake / Twilight Sedation
Fear of general anaesthesia is a common barrier for UK patients. For suitable candidates and appropriate techniques, awake / twilight sedation with local anaesthetic can offer a comfortable experience while avoiding the deeper recovery often associated with general anaesthesia.
Not everyone is a candidate for this approach, and we do not force a one-size-fits-all method. The decision depends on your medical profile, anxiety level, and the complexity of the plan.
What is local anaesthetic with twilight sedation (Conscious Sedation)?
Local anaesthetic numbs the surgical area. Twilight sedation helps you feel calm and relaxed. Many patients describe it as “drifting” or feeling drowsy, with little memory of the procedure. Throughout, vital signs are monitored carefully.
Comfort and control: why it can feel less intimidating
Patients often choose this approach because:
- it can reduce anxiety about “going under”
- post-op grogginess may be milder
- you may feel more in control of the overall experience
We still treat this as real surgery with real standards: proper monitoring, sterile theatres, and clear safety protocols.
Setting realistic expectations: “walk-in, walk-out” without hype
It is tempting for clinics to oversimplify. The truth is more responsible: even with twilight sedation, you will still need rest, compression, and structured aftercare. The benefit is not “no recovery”. The benefit is often a smoother experience for the right patient.
Awake or twilight approaches can reduce fear for many men — but the standard remains the same: safety, precision, and a carefully supported recovery.
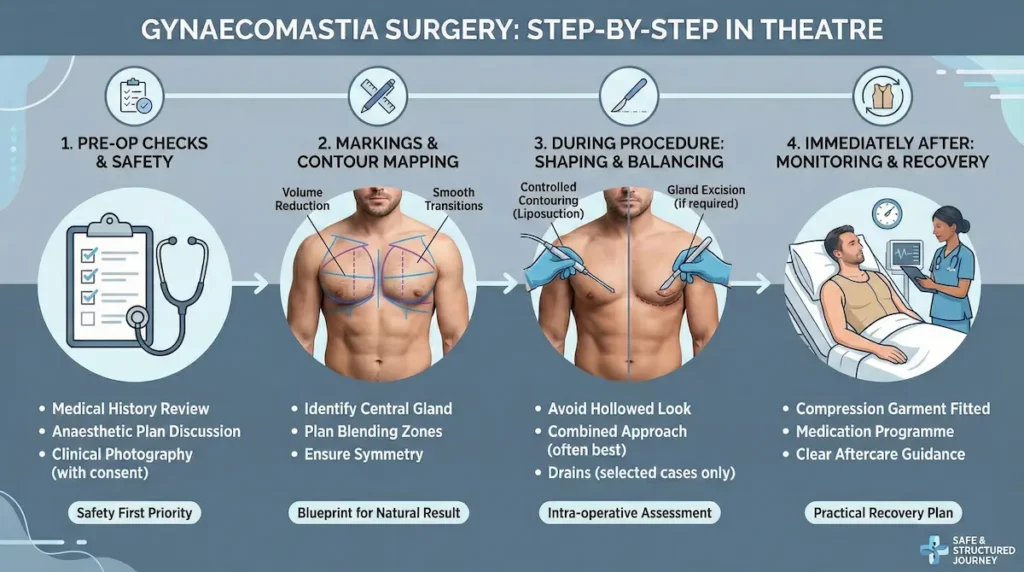
Gynaecomastia Surgery Step-by-Step: What Happens In Theatre?
A well-run treatment day should feel structured and predictable. The details vary depending on whether your plan is liposuction-only, excision, or a combined approach, but the principles are consistent: confirm suitability, mark accurately, maintain sterile technique, and ensure you leave with clear aftercare guidance.
Pre-op checks: safety first, always
Before going to theatre, we confirm key details: your medical history, current medications, allergies, and any recent changes in symptoms. If anything suggests you need further medical review (for example, a new lump or unusual discharge), that takes priority over scheduling.
- Review of medical history and medication list
- Discussion of anaesthetic plan and comfort measures
- Photographic documentation for clinical planning (with consent)
Markings and “contour mapping”
Markings are not just lines on skin. They are the blueprint for a natural result. We map where volume needs reducing, where blending must be gentle, and how the nipple-areola area should sit at rest.
- Identify the central gland zone (if present)
- Plan smooth transitions across the lower and lateral chest
- Consider symmetry and body frame proportions
During the procedure: shaping and balancing
If liposuction is part of your plan, the goal is controlled contouring rather than aggressive removal. If gland excision is required, it is performed with careful judgement to avoid a hollowed look under the areola. In many mixed cases, the combined approach is what creates the most believable male chest contour.
Some patients ask about drains. They may be used in selected cases where fluid management is a concern, but they are not automatically required for everyone. The decision is based on your tissue pattern, grade, and intra-operative assessment.
Immediately after: monitoring, garment, and discharge guidance
After the procedure, you are monitored while the initial swelling and comfort levels stabilise. You will be fitted into a compression garment and given a practical recovery plan (movement, hygiene, sleeping position, and warning signs to watch for).
- Compression garment fitted and explained
- Medication plan (pain control and any prescribed support)
- Clear do’s and don’ts for the first week
The procedure is only one part of the outcome. The other part is your recovery plan — structured, realistic, and followed properly.
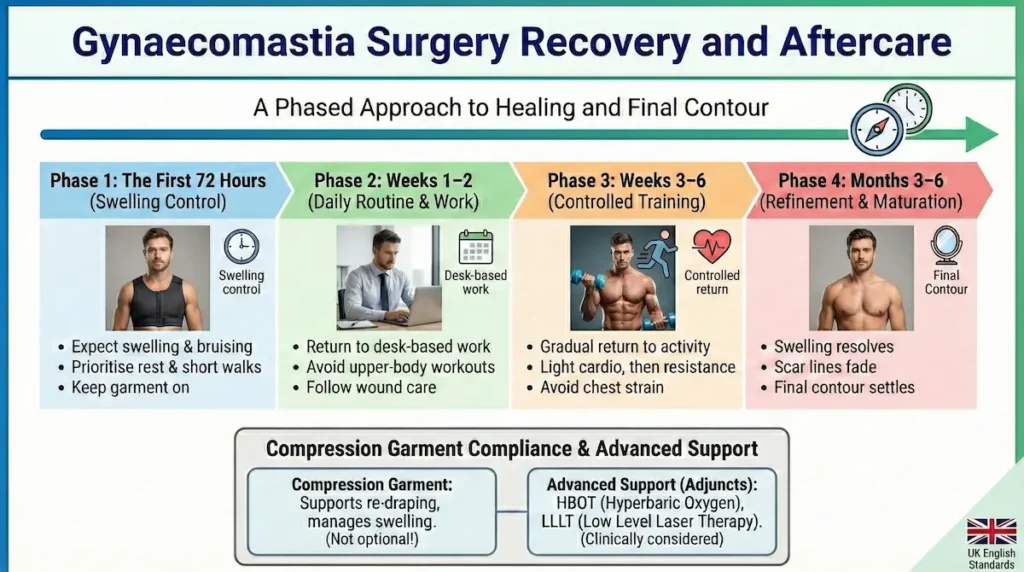
Gynaecomastia Surgery Recovery and Aftercare
Healing happens in phases. Early on, swelling and bruising can make the chest look uneven or “not finished”. That is normal. Most men feel socially comfortable fairly quickly, but the final contour and scar maturation take longer. If you are travelling back to the UK, your plan should include sensible timing, movement, and follow-up structure.
The first 72 hours: swelling control and sensible movement
The early phase is about comfort, rest, and avoiding unnecessary strain. Gentle walking is encouraged to support circulation, but heavy lifting and intense activity are avoided.
- Expect swelling, tightness, and bruising
- Prioritise sleep, hydration, and short walks
- Keep the garment on as instructed
Weeks 1–2: daily routine, work, and “looking normal” in clothing
Many patients can return to desk-based work within 7–14 days, depending on comfort and job demands. The chest will still be settling, but most men feel significantly more comfortable in everyday clothing during this phase.
- Walking is fine; avoid upper-body workouts
- Driving depends on comfort and safe movement
- Follow wound care guidance precisely
Weeks 3–6: controlled return to training
This is where patience pays off. Rushing back to heavy chest training too early can prolong swelling or irritate healing tissue. We generally guide a gradual return, starting with lower-impact activity and progressing as your recovery allows.
- Light cardio first, then progressive resistance
- Avoid direct chest strain until cleared
- Continue garment use if advised
Months 3–6: refinement, scar maturation, and the final contour
By this stage, most swelling has resolved and the chest looks increasingly “settled”. Scar lines often fade and soften progressively, though full maturation can continue up to 12 months.
Compression garment compliance: the unglamorous detail that protects results
The compression garment is not optional “extras”. It helps manage swelling, supports skin re-draping, and can reduce the risk of fluid build-up. Wearing it exactly as instructed is one of the most controllable factors you have.
Advanced recovery support: HBOT and LLLT (when clinically appropriate)
Some patients ask how to reduce downtime and return to normal life sooner. Where suitable, supportive recovery technologies may be used as part of a broader aftercare plan:
- HBOT (Hyperbaric Oxygen Therapy): involves breathing oxygen in a controlled environment. In selected cases, it may support tissue recovery by optimising oxygen delivery during healing.
- LLLT (Low Level Laser Therapy): a non-invasive therapy that may help reduce inflammation and support tissue repair in certain recovery protocols.
These are adjuncts, not shortcuts. They do not replace good surgical planning or proper aftercare. They may be considered based on your clinical profile and recovery goals.
Fast recovery is not about rushing. It is about doing the basics consistently — and using supportive protocols only when they genuinely fit your case.
Safety And Risks: Is Gynaecomastia Dangerous?
Any surgical procedure carries risk, and it is important to discuss this plainly. The aim is not to promise “zero risk”, but to reduce risk through proper patient selection, careful technique, and structured aftercare.
Common risks (and what they look like)
- Swelling and bruising: expected early on and gradually improves.
- Seroma (fluid build-up): may require monitoring and, in some cases, drainage.
- Haematoma (bleeding collection): uncommon but can require prompt assessment.
- Infection: risk is reduced with sterile technique and proper wound care.
Contour and symmetry risks
Even with excellent technique, the chest can heal unevenly early on due to swelling. Longer-term concerns may include minor asymmetry, contour irregularity, or persistent puffiness if glandular tissue was not adequately addressed. This is why correct tissue diagnosis and a tailored plan matter so much.
Sensation changes and scar-related issues
Temporary changes in nipple-areola sensation can occur, and scars can thicken in some skin types. We plan incisions carefully and guide scar aftercare, but biology still plays a role in how scars mature.
How risk is reduced: the practical checklist
- Appropriate pre-op assessment and sensible patient selection
- Careful technique focused on natural contour, not aggressive removal
- Structured aftercare: garment use, activity limits, and follow-up
- Clear guidance on warning signs and when to seek review
Is Gynaecomastia Surgery Safe In Turkey for UK Patients?
For UK patients, the real question is not “Turkey vs UK” as a headline. It is: who is treating you, what standards are in place, and how consistently are they applied? Safety comes from clinical governance — appropriate assessment, sterile theatres, proper monitoring, and a recovery plan that does not end when you leave the building.
Travelling for surgery can be safe when the pathway is designed for international patients: clear pre-op screening, a structured in-country recovery window, and organised follow-up once you return home.
NHS eligibility vs private: why many men look abroad
In the UK, access can be shaped by eligibility criteria, long waiting times, and variable pathways. Some men are told their case is not covered, while others face delays that feel disproportionate to how much the condition affects daily life.
For many, private care is the next step — but private pricing and availability can be a barrier. This is why some UK patients explore international options: not because they want “cheap”, but because they want a predictable timeline and a comprehensive plan.
What “UK-standard safety” actually means (beyond marketing)
When you compare providers, focus on specifics rather than slogans. A safe pathway typically includes:
- proper medical history review, medication screening, and suitability checks
- a clearly explained anaesthesia plan (including who monitors you)
- sterile operating theatres and standardised infection control
- structured aftercare, compression guidance, and clear warning signs
- realistic travel planning (not rushing you onto a flight too soon)
If a clinic cannot explain these points plainly, treat that as a warning sign.
Travel logistics: how to reduce risk when you fly back to the UK
Travel is not an afterthought. It is part of the medical plan. We advise UK patients to:
- build in adequate local recovery time before flying
- stay mobile with gentle walking (as advised) to support circulation
- follow hydration and garment guidance carefully
- know exactly who to contact if you notice swelling, fluid build-up, or increasing pain
Safety is a pathway, not a postcode: the right assessment, the right technique, and the right aftercare make the difference.

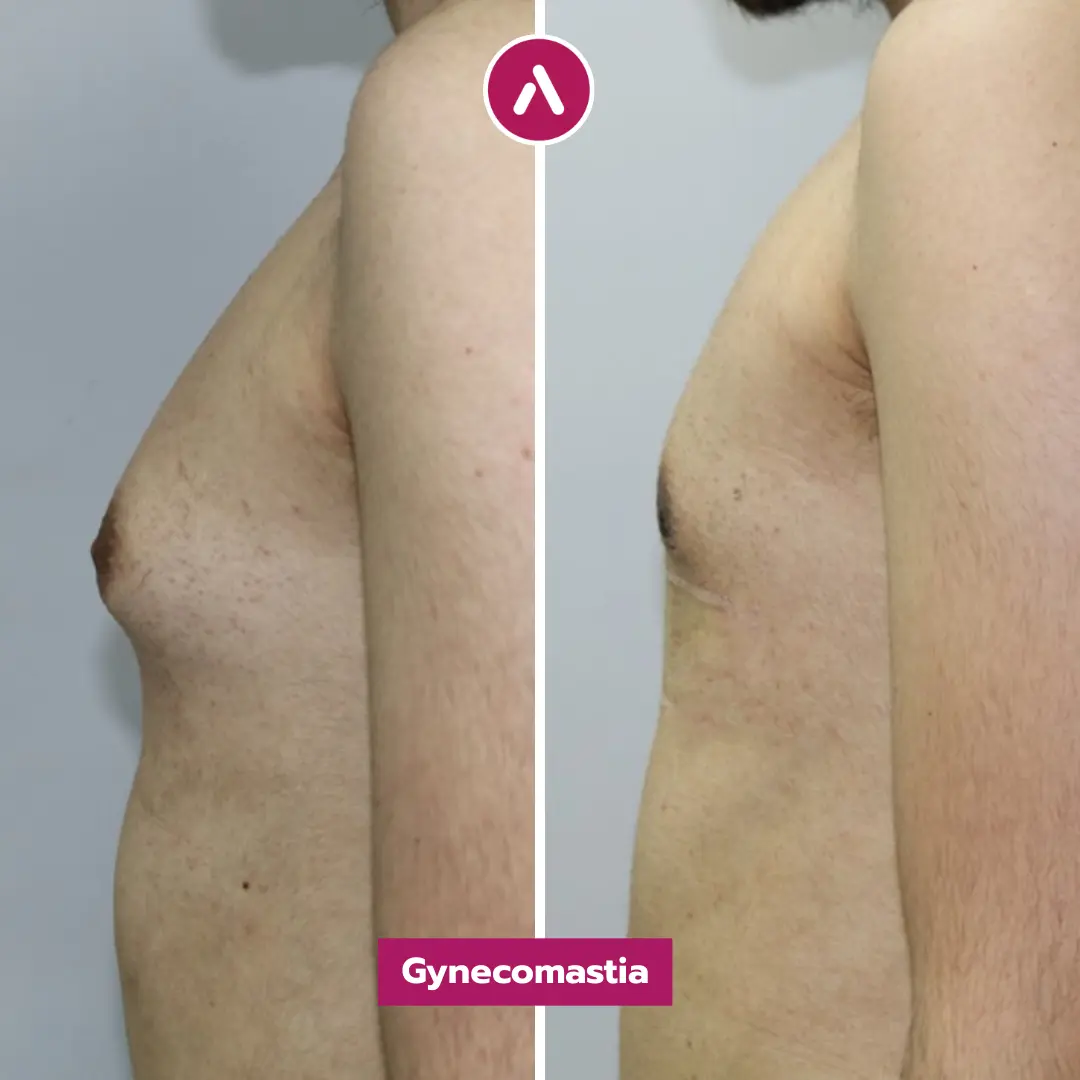
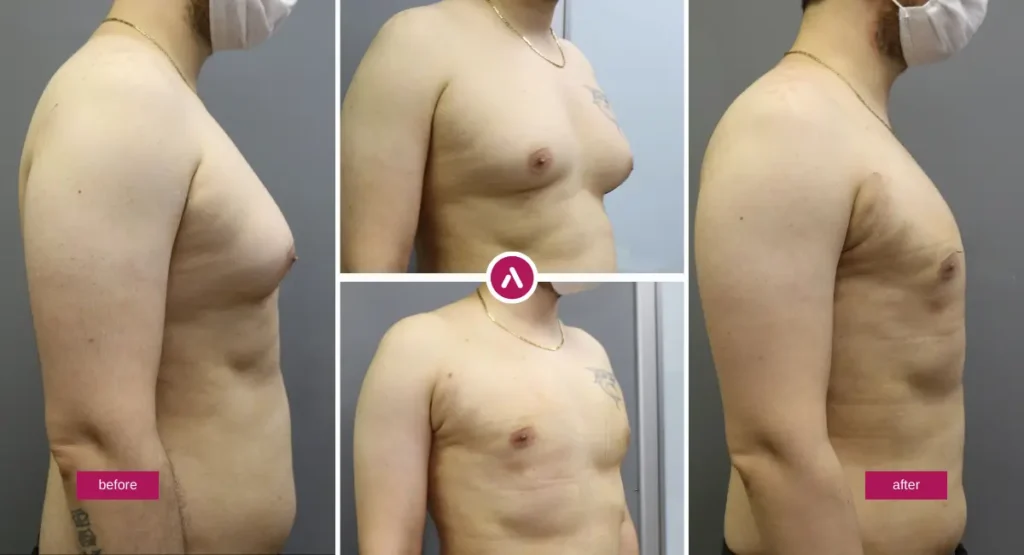
Male Breast Reduction Before and After: Realistic Expectations and Results
The best outcomes are both physical and psychological: a chest that feels normal to live in, not something you manage every day. At the same time, the healing process is not instant. Swelling, firmness, and temporary asymmetry are common early on, and the chest continues refining for months.
What you may see early vs what you see later
- First 2–4 weeks: swelling, bruising, and tightness can distort contour.
- Weeks 6–12: the chest typically looks more settled; garment compliance pays off.
- Months 3–6: refinement becomes clearer; scars often soften and fade.
- Up to 12 months: scar maturation continues and the final “quiet” result emerges.
It is normal for one side to settle faster than the other. Healing is rarely perfectly symmetrical week to week.
Will it come back?
Recurrence is uncommon when true glandular tissue has been removed appropriately, but future changes are still influenced by biology and lifestyle. Weight gain can add chest fat. Certain medications or hormone-related factors can contribute to tissue changes again. That is why we take history seriously and talk about triggers openly.
How “flat” is too flat? (avoiding the hollowed look)
Many men want certainty: “remove everything.” A natural male chest still has a small, normal thickness under the areola. Over-resection can create indentations that look unnatural, especially in certain lighting or when raising the arms. Our aim is a balanced contour: flat enough to look masculine, not so aggressive that it looks surgical.
Revision: when is it considered?
Most patients do not need revision. If a concern persists after the chest has fully settled, it is assessed objectively. Common reasons for review include persistent puffiness, contour irregularity, or noticeable asymmetry that does not improve after swelling resolves.
Judge results on a realistic timeline. Early swelling can be loud; the final result is quieter and more natural.
Gynaecomastia Surgery Cost 2026: Turkey vs UK
UK patients frequently search for gynaecomastia surgery cost UK vs Turkey. The most honest answer is that cost depends on your grade, tissue type, technique (liposuction, gland excision, or combined), and whether additional recovery support is included. Instead of chasing a single number, compare what is actually provided and how that affects safety and predictability.
What drives the price in any country?
- Complexity: grade, skin excess, and whether gland removal is required
- Time and technique: combined contouring is more technical than a single step
- Anaesthesia and monitoring: the plan should match your medical profile
- Aftercare structure: follow-up, garments, and support protocols
- Reputation and experience: surgeon expertise and consistent outcomes
UK private vs all-inclusive travel pathways: what to compare
Some UK clinics price the surgery itself, with add-ons charged separately. Many international pathways package logistics so your medical journey is more predictable. For example, a patient may compare male breast reduction cost London vs Istanbul and find that the difference is not only the surgeon’s fee, but also what is included around it (tests, accommodation, transfers, and aftercare support).
| Comparison point | Typical UK private pathway | Typical all-inclusive pathway (Istanbul) | Why it matters |
|---|---|---|---|
| Pricing structure | Surgery fee + separate add-ons | Often packaged for predictability | Helps you compare like-for-like, not headline prices |
| What is included | Varies: tests, garments, follow-up may be separate | Often includes transfers, accommodation, medications, garment, scheduled follow-up | Hidden extras can change the real total cost |
| Timeline | Dependent on clinic capacity and scheduling | Often faster scheduling once suitable | Time-to-treatment can be a major decision factor |
| Aftercare pathway | Usually local follow-up appointments | In-country checks + remote follow-up after you return | Continuity of care is a safety issue, not a luxury |
| Travel planning | Not applicable | Must be integrated into the medical plan | Reduces risk when the flight home is managed sensibly |
How to choose based on value (not “cheap vs expensive”)
For an “expert patient”, the best decision is rarely the lowest price. It is the plan that is medically sound, aesthetically precise, and supported properly — with clear answers to questions about technique, safety, and follow-up.

Finding The Best Gynaecomastia surgeon: What UK Patients Should Look For
If you are comparing options, the most useful approach is to ask questions that reveal judgement and process — not just promises. A good surgeon will explain your tissue type, show how they plan scars and contour, and give a recovery plan that fits your work and travel reality.
Credentials and scope: who is actually doing what?
Ask who performs each part of your care, and how they work as a team. The safest pathways are clear about roles, accountability, and follow-up.
- Who is the operating surgeon, and what is their focus in male chest contouring?
- Who monitors you during anaesthesia or sedation, and what is the protocol?
- What is the clinic’s plan for post-op reviews and remote follow-up once you return to the UK?
Questions that reveal technique (and prevent “lipo-only disappointment”)
Many revision enquiries start with the same story: “I had liposuction, but the puffy area remained.” If you suspect a gland component, these questions matter.
- Do you think my case is fat, gland, or mixed — and why?
- If there is gland, will you remove it directly (and how do you avoid a hollowed look)?
- How do you blend the chest contour so the result looks natural in movement?
Red flags: what should make you pause?
- Guaranteed outcomes, “no risks”, or pressure to book immediately
- No clear explanation of technique choice (especially gland vs fat)
- Vague aftercare plans, or no structured follow-up once you travel home
Choose the surgeon who can explain your plan calmly and specifically — not the one who promises the most.
Your Medical Journey With Us (designed for UK patients)
This section is intentionally brief. The clinical parts matter most. Still, international treatment should feel organised, not improvised. For UK patients, the goal is a predictable pathway: clear pre-op assessment, a structured in-country recovery window, and organised follow-up once you are home.
Remote review and planning before you travel
We typically begin with a clinical review of your history and goals, then discuss whether your chest looks more consistent with fat, gland, or a mixed pattern. If anything suggests you should see your GP first (for example, a new lump or worrying symptoms), we will say so.
Travel logistics and comfort: keeping it simple and structured
International patients often prefer an organised plan that reduces friction. Where appropriate, this may include:
- airport transfers and local transport coordination
- hotel accommodation planning during the early recovery phase
- compression garment and medication guidance as part of aftercare
Follow-up after you return to the UK
Continuity of care matters. Your plan should include scheduled check-ins and a clear route for questions such as swelling, fluid build-up, or scar concerns. If you need an in-person assessment in the UK for any reason, we will advise you appropriately.
Conclusion
Gynaecomastia Surgery can be life-changing in a quiet, practical way: clothes fit better, posture improves, and the chest stops dominating your attention. The best outcomes come from accurate diagnosis (fat vs gland vs mixed), a technique chosen for your anatomy, and a recovery plan you can realistically follow — especially if you are travelling from the UK.
If you would like a clinical opinion on whether your case is more consistent with fat, gland, or both, you can request an assessment and receive a clear, medically grounded plan.
Gynaecomastia (Male Breast Reduction) Frequently Asked Questions (FAQ):
How do I know if I have “moobs” or true gynaecomastia?
The appearance can be similar. True gynaecomastia often includes a firmer subareolar disc, while chest fat is softer and more diffuse. A clinical assessment is the most reliable way to confirm tissue type.
Gynaecomastia vs chest fat: does weight loss fix it?
Weight loss can reduce fat, but it typically does not remove dense glandular tissue. If your chest remains “puffy” at a stable weight, gland may be part of the cause.
Do I need gland removal, or is liposuction enough?
If the problem is mainly fat and the skin recoils well, liposuction may be sufficient. If there is a firm gland behind the areola, excision is often needed to avoid residual puffiness. Many cases benefit from a combined approach.
Will the gland come back after surgery?
Recurrence is uncommon when glandular tissue is removed appropriately. However, future weight gain, hormone changes, or medication triggers can affect the chest again, mainly through fat or new tissue stimulation in susceptible cases.
Is the procedure painful?
Most patients describe tightness, soreness, and bruising rather than severe pain. Discomfort is usually most noticeable in the first few days and improves steadily with the recommended pain-control plan.
How long will I need off work?
Many men return to desk-based work in around 7–14 days, depending on comfort and the demands of their job. Physically demanding roles often need a longer break. Training and heavy lifting are reintroduced gradually.
Do I need drains?
Not always. Drains may be used in selected cases depending on tissue pattern, grade, and intra-operative judgement. The goal is to reduce fluid build-up risk while keeping recovery practical.
Will I have visible scars?
Most scars are designed to be discreet, commonly around the edge of the areola and/or tiny liposuction access points. Scar visibility depends on skin type and healing biology, and scars typically mature over months.
When can I fly back to the UK?
Flying is part of the medical plan. You should build in adequate local recovery time, follow mobility and hydration guidance, and know what warning signs to watch for. Your surgeon’s advice should be individual to your case.
Can the chest look uneven at first?
Yes. Early swelling can be asymmetrical, and one side often settles faster. This is common in the first weeks. The more meaningful judgement point is usually later, once swelling has reduced.
Why do some UK patients consider surgery abroad rather than the NHS?
In the UK, access can be influenced by eligibility criteria and waiting times, and some cases are not covered. Many men then compare private options. Others prefer an international pathway for a predictable schedule and an all-in-one plan — provided safety and follow-up are clear.
What if I need a revision?
Most patients do not. If a concern persists after the chest has fully settled, it should be assessed objectively. Revision decisions are typically considered only after adequate healing time.
Can gynecomastia surgery be done if I am very lean?
Yes. In lean patients, gynecomastia is often driven more by glandular tissue than fat, so precise gland reduction and careful contour blending are essential to avoid an over-resected, hollow look.
Does gynecomastia affect nipple shape or areola size?
It can. Gynecomastia may make the areola look puffy or more prominent. A tailored plan focuses on flattening the subareolar profile while maintaining a natural nipple-areola contour as swelling settles.
Is gynecomastia linked to testosterone levels?
Sometimes. Gynecomastia can be influenced by the balance between androgens and oestrogens, but it is not always a simple “low testosterone” issue. If symptoms suggest a hormonal trigger, a medical assessment and blood tests may be appropriate before treatment planning.
How is gynaecomastia different from man boobs caused by weight gain?
Gynaecomastia involves true glandular tissue, while man boobs from weight gain are often primarily fat (pseudogynecomastia). Many men have a mix of both, which is why the treatment plan must be based on tissue type rather than appearance alone.
Can gynecomastia return if I lose and regain weight (the “yo-yo” effect)?
Weight changes can affect chest fat and make the chest look fuller again, even after gynecomastia treatment. If the original problem included a gland and it was removed appropriately, true gland recurrence is uncommon, but maintaining a stable weight helps protect the overall contour. If man boobs were partly fat-driven, weight regain can be more noticeable.
Medical disclaimer: This page provides general information and does not replace a consultation with a qualified clinician. Suitability, risks, and expected outcomes vary by individual. If you have a new lump, nipple discharge, rapid changes, or significant pain, seek medical assessment promptly.








