
If you’re researching diastasis recti repair surgery, you’re likely trying to answer two questions at once: Is this a medical problem that needs treatment, a cosmetic concern, or both? For many “expert patients,” the decision isn’t about vanity—it’s about function, comfort, confidence, and minimizing risk with a plan that is grounded in medical science and realistic outcomes.
In this guide, we’ll break down what diastasis recti is, how it’s assessed, what non-surgical care can and can’t do, and what surgery to repair diastasis recti typically involves. We’ll also cover key topics people search for—like diastasis recti repair surgery recovery, diastasis recti repair surgery cost, and what “before and after” photos can (and cannot) prove.
Key takeaway: Diastasis recti isn’t always “just cosmetic.” In some patients it contributes to core instability, discomfort, and limitations in daily movement—while in others, it’s primarily an aesthetic contour issue. Many cases sit in the middle.
Table of Contents
What Is Diastasis Recti and Why It Matters Beyond “Looks”
Diastasis recti refers to a widening of the connective tissue (the linea alba) between the left and right rectus abdominis muscles—often described as “abdominal muscle separation.” While the visual “bulge” can be the most noticeable sign, the real impact is often functional: changes in pressure management, core stability, and how the abdominal wall supports your spine and pelvis. Understanding the basics helps you evaluate whether diastasis recti muscle repair surgery is appropriate, or whether targeted rehabilitation may be enough.
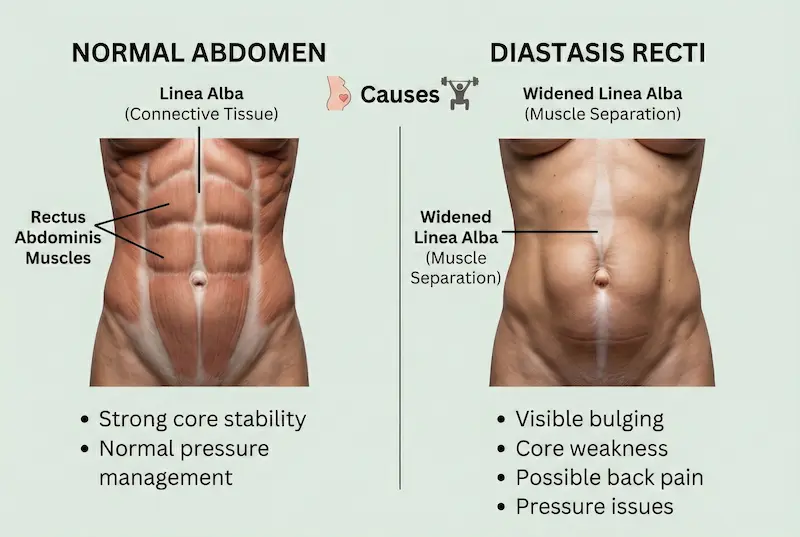
The anatomy: linea alba, rectus muscles, and “muscle separation”
The rectus abdominis muscles (“six-pack” muscles) sit on either side of the midline. The linea alba is the collagen-rich structure that connects them. In diastasis recti, this midline tissue becomes stretched and thinned, which can reduce the abdominal wall’s ability to transmit force efficiently. In simple terms: the issue is not that the muscles are “torn,” but that the connective tissue between them has widened and weakened.
Common causes (pregnancy, weight changes, genetics, prior abdominal surgery)
Pregnancy is the most common cause, but diastasis recti can also occur with major weight fluctuations, repetitive heavy lifting with poor pressure control, connective tissue predisposition, or after abdominal surgeries. Severity varies widely. Some people recover significantly with appropriate rehab; others continue to experience bulging or functional symptoms despite consistent training.
Postpartum diastasis rarely shows up alone. The same pregnancy and weight-fluctuation cycle that stretches the linea alba often also produces breast volume changes, abdominal skin laxity, and a “pooch” that fitness alone cannot resolve. For many postpartum patients, addressing these together—rather than as separate procedures over multiple recovery cycles—is the more practical surgical conversation.
The combined-procedure planning logic, candidacy criteria, and recovery overview specific to postpartum patients are detailed in our mommy makeover overview.
Symptoms that signal a functional problem (core weakness, back pain, bulging)
Not everyone with diastasis recti has symptoms. When symptoms occur, they may include visible midline bulging during exertion, a sense of core weakness, difficulty with certain movements, posture strain, and low back discomfort. Some patients also report challenges with pressure management during exercise. A skilled evaluation matters because symptoms can overlap with hernias, pelvic floor dysfunction, or general deconditioning.
Medical vs Cosmetic: When Diastasis Recti Repair Surgery Is Functional, Aesthetic—or Both
Patients often assume there’s a strict line between “medical” and “cosmetic,” but real-life cases are nuanced. A person may want improved contour and better core function. Another may have minimal cosmetic concern but significant limitations during activity. This is why thorough assessment and clear goal-setting are essential before deciding on diastasis recti surgery repair or any repair diastasis recti surgery plan.
Functional goals: core stability, posture, pain reduction, exercise tolerance
From a functional standpoint, repair aims to restore the abdominal wall’s mechanical integrity—improving how forces transfer through the torso. In properly selected patients, this can support better trunk stability and reduce the “doming” that occurs during effort. However, outcomes depend on your baseline condition, any coexisting hernia, your rehabilitation plan, and surgical technique. Good care is built on what scientific research shows about biomechanics and patient-reported outcomes—not just marketing claims.
Cosmetic goals: abdominal contour, waist definition, “pooch” improvement
From an aesthetic standpoint, patients commonly seek a flatter abdomen, improved waist definition, and reduced lower abdominal protrusion. It’s important to distinguish contour changes caused by skin laxity and fat distribution versus changes caused by diastasis. This is also where diastasis recti repair surgery before and after galleries can be informative—but only if they show comparable lighting, posture, and time-from-surgery, and if the patient had similar anatomy to yours.
How surgeons evaluate “medical necessity” vs “cosmetic preference”
Clinically, evaluation typically considers symptom burden, functional limitation, and whether non-surgical management was attempted. Surgeons will also assess for an associated hernia, abdominal wall laxity, and skin excess. Importantly, “medical” and “cosmetic” motivations can coexist—your plan should match your priorities while staying conservative on risk. (Later in this article, we’ll detail how this impacts technique selection, diastasis recti repair surgery cost, and diastasis recti repair surgery recovery.)

How Diastasis Recti Is Diagnosed and Graded
A reliable diagnosis is the foundation of any safe plan—especially if you’re comparing diastasis recti repair surgery options or trying to decide whether you truly need surgery to repair diastasis recti. Because abdominal “bulging” can come from multiple causes (including hernias), grading should be done by an experienced clinician who can assess the abdominal wall under controlled conditions and rule out red flags.
Self-checks vs clinical examination: what’s reliable and what isn’t
At-home checks can help you notice a pattern (for example, doming during a crunch or getting out of bed), but they are not a definitive diagnosis. Clinical exams typically evaluate the width and quality of the midline tissue (linea alba), how the abdominal wall behaves under tension, and whether symptoms correlate with movement. Self-checks can be misleading if you have significant subcutaneous fat, posture-related anterior pelvic tilt, or a small hernia that “mimics” diastasis.
Imaging options (ultrasound/CT) and when they’re useful
Imaging is not always necessary, but it can be useful when the physical exam is unclear, when symptoms suggest a hernia, or when surgical planning requires additional detail. Ultrasound can dynamically assess midline widening and tissue quality during movement, while CT may be considered when a hernia is suspected or when there’s complex anatomy from previous surgery. The goal is precision—good outcomes depend on aligning technique with anatomy, a principle supported by medical science and surgical outcome research.
Severity, hernias, and red flags that change the treatment plan
Severity isn’t only “how many fingers wide” the gap feels. Clinicians consider width, length, tissue tension, and whether there is a concurrent umbilical/ventral hernia. Red flags that should trigger prompt medical evaluation include severe or worsening pain, a firm irreducible bulge, nausea/vomiting with a bulge, or signs of bowel obstruction. These are not typical “cosmetic diastasis” features and can change the urgency and type of repair.
| What’s Being Assessed | Why It Matters | How It Influences Treatment |
|---|---|---|
| Width & length of separation | Measures extent of midline laxity | Guides whether rehab may be sufficient vs surgical repair |
| Quality/tension of linea alba | Indicates strength of connective tissue | May impact durability of repair and technique choice |
| Associated hernia (umbilical/ventral) | Hernias can cause symptoms and risk complications | May require hernia-specific repair strategy |
| Skin excess & fat distribution | Major drivers of contour outcome | Helps decide standalone repair vs abdominoplasty-based approach |
| Functional symptoms (pain, instability) | Clarifies “medical vs cosmetic” motivations | Supports a plan that prioritizes function and safety |
Non-Surgical Treatment First: What Can (and Can’t) Be Fixed Without Surgery
Many patients do not need surgery immediately—and some never need it. A structured rehabilitation program can improve control of intra-abdominal pressure, reduce doming, and enhance functional strength. However, it’s equally important to understand the limits: non-surgical care may improve function and appearance, but it cannot always fully restore stretched connective tissue. If you’ve tried high-quality rehab and still have persistent bulging or functional impairment, that’s often when people start researching diastasis recti muscle repair surgery and diastasis recti surgery repair in a more serious way.
Physical therapy and core rehab: realistic expectations and timelines
A good program is typically guided by a clinician experienced in postpartum/core rehabilitation and focuses on breathing mechanics, pressure management, and progressive strengthening—not endless crunches. Many people notice improvements over weeks to months, especially in stability and how the abdomen behaves during movement. The key is progression and form. In scientific research on core rehabilitation, better outcomes generally correlate with consistency, correct technique, and individualized loading rather than one-size-fits-all routines.
Bracing, lifestyle adjustments, and training modifications
Temporary bracing may help some patients feel supported early on, but it shouldn’t replace active rehabilitation. Training modifications can be particularly important: exercises that increase pressure dramatically (improper heavy lifting, aggressive sit-ups, certain planks if done with poor control) may worsen doming. Lifestyle factors like constipation management and safe lifting strategies can also reduce repeated strain on the midline.
When conservative treatment isn’t enough (criteria that push toward surgery)
Consider a surgical consultation when you have persistent bulging or doming despite a structured rehab plan, ongoing functional limitations (e.g., difficulty with daily activities or exercise), significant discomfort, or a confirmed hernia. At that stage, the conversation often shifts from “Can I avoid surgery?” to “Which option is safest and most predictable?”—including whether you need a standalone repair or a procedure that also addresses skin laxity for cosmetic goals.
Practical guidance: Before deciding on repair diastasis recti surgery, ask yourself: “Have I completed a structured rehab plan for long enough to judge results?” If yes—and symptoms or bulging persist—then a surgical evaluation becomes reasonable.
Surgical Techniques for Diastasis Recti Repair Surgery
When conservative treatment isn’t enough, diastasis recti repair surgery is typically designed to restore midline support by bringing the rectus muscles back toward the center (usually with a technique called plication). The “best” operation isn’t universal—it depends on whether your main issue is functional instability, contour/skin excess, an associated hernia, or a combination. In other words, diastasis recti surgery repair is a spectrum of approaches, not a single standardized operation.
Suture plication: how the repair is performed and who it fits best
In most cases, the core of diastasis recti muscle repair surgery is suture plication—the surgeon places strong sutures to tighten and reinforce the stretched linea alba, narrowing the midline and improving abdominal wall mechanics. This can be done as part of a tummy tuck (abdominoplasty) or, in selected cases, as a more limited repair. People who benefit most are those with persistent bulging/doming, core weakness, and lax midline tissue despite good rehab.
However, plication does not “create a six-pack,” and it cannot substitute for overall conditioning. Good surgeons set expectations clearly: surgery to repair diastasis recti addresses structure; long-term results also depend on weight stability, safe lifting mechanics, and a rehab plan that protects the repair while rebuilding strength.
One detail rarely covered upfront: anesthesia choice changes the recovery curve more than most patients expect. For limited plication or selected combined repairs, awake protocols using tumescent anesthesia and light sedation are an option in carefully chosen candidates. The trade-off is reduced general-anesthesia exposure versus a different intra-operative experience and stricter candidacy criteria.
The full awake protocol mechanics, candidacy framework, and how the recovery profile shifts compared to general anesthesia are detailed in our awake tummy tuck primer.



Mesh vs no mesh: when reinforcement is considered and why
Most diastasis repairs do not automatically require mesh. Mesh may be considered when there is a concurrent ventral/umbilical hernia, when tissue quality is poor, or when the surgeon feels reinforcement improves durability. The decision is individualized and should be explained in plain language: what problem mesh is solving, where it will be placed, and what trade-offs exist (for example, the balance between reinforcement and potential mesh-related complications).
If you’re comparing options, ask your surgeon to explain the plan as if they’re teaching it: “Is this a plication-only repair, or is it a hernia repair plus diastasis repair?” That distinction often matters more than marketing labels.
Tummy tuck (abdominoplasty) vs standalone repair: choosing the right approach
Many patients discover that their “diastasis problem” includes a skin component. If you have significant loose skin, stretch marks below the navel, or laxity that affects contour, the most predictable aesthetic improvement often comes when repair diastasis recti surgery is combined with abdominoplasty. If your skin is tight and your goal is primarily functional, a standalone repair may be discussed (depending on anatomy and surgeon preference).
| Option | Best For | What It Typically Addresses | What It May Not Fix |
|---|---|---|---|
| Standalone diastasis repair | Primarily functional instability with minimal skin excess | Midline tightening (plication) to improve support | Loose skin, significant contour issues from skin laxity |
| Tummy tuck + diastasis repair | Diastasis + loose skin/stretch marks (often postpartum or after weight change) | Midline repair + skin tightening/removal for contour | Doesn’t “replace” fitness; weight changes can affect results |
| Tummy tuck + lipo (selected cases) | When fat distribution also contributes to contour concerns | More comprehensive shaping (surgeon-dependent) | Not ideal for everyone; safety depends on scope and health status |
The standalone-vs-combined choice often gets oversimplified at consultation.
For most patients with both midline laxity and skin component, the combined approach delivers a more predictable contour outcome—but the operation, recovery, and risk profile differ meaningfully from a limited plication. The right answer depends on whether your priority is structural repair, contour, or both.
The full procedural mechanics, technique variations, recovery framework, and pricing context for the combined approach are detailed in our tummy tuck surgical reference.
Diastasis Recti Repair Surgery Cost: What Drives Pricing (and Why Quotes Vary So Much)
Searching diastasis recti repair surgery cost can be frustrating because prices vary widely based on geography, facility fees, anesthesia, whether a tummy tuck is included, surgeon experience, and whether a hernia repair is also needed. The most reliable way to interpret cost is to compare “like for like”: standalone repair vs tummy tuck-based repair, and what is included (anesthesia, operating room, garments, aftercare, and follow-ups).
Below is a practical, research-informed way to think about cost ranges. The U.S. national average surgeon’s fee for a tummy tuck is reported by the American Society of Plastic Surgeons (ASPS), while RealSelf aggregates patient-reported averages by metro area; these sources show how dramatically costs can shift by city. For medical tourism destinations, publicly listed package estimates exist, but you should treat them as starting points and verify what’s included.
| Location | Typical Reported Price Context | What This Usually Reflects |
|---|---|---|
| United States (national) | ASPS reported average surgeon’s fee for tummy tuck | Surgeon’s fee only (often excludes anesthesia & facility) |
| Los Angeles | RealSelf metro average is higher than many regions | High-demand metro pricing; scope and inclusions vary |
| Miami | RealSelf metro average is often lower than LA/NYC | Competitive market; still varies by safety standards and complexity |
| Istanbul (Turkey) | Published package estimates exist online | Often bundles surgery + hospital stay and sometimes logistics; confirm exact inclusions |
| Mexico / Thailand | Published ranges and package estimates exist | May appear attractive; evaluate surgeon credentials, facility standards, and aftercare carefully |
The U.S. metro tables and destination-package estimates are reference points—they’re not a methodology. Comparing across borders responsibly means weighing surgeon-specific volume, facility accreditation, anesthesia infrastructure, aftercare continuity, and complication-pathway logistics—each of which moves the real “value” calculation independently of the headline price. A cheaper quote with weaker infrastructure isn’t a saving; it’s a deferred cost.
The full international comparison methodology, including the structural factors that determine which “package” actually represents value, is in our international clinic vetting reference.
Reference points (not personal quotes): ASPS reports an average tummy tuck surgeon’s fee in the U.S. (excluding anesthesia/facility). RealSelf reports an overall average and metro averages (including Los Angeles and Miami). Published estimates for Istanbul, Mexico, and Thailand vary by clinic and what’s included, so always request a line-item breakdown and confirm safety protocols. (Sources: ASPS and RealSelf for U.S. averages; published destination estimates for Istanbul/Mexico/Thailand.)

What to Expect: Diastasis Recti Repair Surgery Recovery Timeline, Activity Restrictions, and Scar Planning
Diastasis recti repair surgery recovery is usually straightforward—but it requires patience and strict respect for lifting limits early on. The most important concept is this: the repair needs time to “hold” while swelling settles and tissues regain strength. A well-structured recovery plan reduces complications (like wound issues or fluid collections) and helps protect long-term results.
Day-by-day and week-by-week recovery milestones
While every surgeon’s protocol is personalized, many postoperative plans follow similar milestones. Multiple clinical sources describe early lifting restrictions and a gradual return to activity, with light activity resuming around the first month and more complete exercise often returning later—commonly in the 6–8 week range, depending on complexity and surgeon clearance.
| Timeframe | What You’ll Likely Be Doing | What You Should Usually Avoid |
|---|---|---|
| Days 1–7 | Walking frequently (short, gentle), focused rest, swelling management | Straining, heavy lifting, “testing” your core, intensive chores |
| Weeks 2–4 | Gradual increase in daily activity; many return to light routines | Heavy lifting; high-pressure core moves; intense cardio without clearance |
| Weeks 4–6 | Many protocols begin easing restrictions; walking and light activity expand | Heavy lifting and aggressive core training unless your surgeon approves |
| Weeks 6–8+ | Often a return toward fuller exercise with clearance; gradual core progression | Jumping back to max lifting or intense ab work without a staged plan |
| Months 3–6 | Continued strength rebuilding; scar maturation; final contour evolving | Major weight swings; ignoring ongoing core mechanics and pressure control |
Note: If your operation combines diastasis recti surgery repair with a tummy tuck or hernia repair, your restrictions may be stricter or last longer than a limited repair.
Compression garments, mobility, and returning to work/exercise safely
Many surgeons recommend compression garments for swelling control and comfort (specific duration varies). Early, frequent walking is often encouraged to support circulation, while core-straining movements are restricted. Return-to-work timing depends on your job demands: desk work can be sooner than physically demanding roles. For exercise, many surgeons advise a staged plan—reintroducing activity gradually and delaying intense core-focused workouts until cleared, which is commonly several weeks post-op.
Scar location, scar care, and factors that influence final appearance
Scar placement depends on the approach. When a tummy tuck is involved, the incision is typically positioned low on the abdomen to be concealed by underwear/swimwear. Scar quality is influenced by genetics, tension on the closure, infection risk, smoking status, and postoperative care. Ask your surgeon what scar care they recommend (silicone therapy is commonly discussed), and remember that scars “mature” over months—not weeks.
“Silicone therapy” gets named in most surgeon recommendations and explained in almost none. The actual scar maturation timeline, when each intervention (silicone sheets, laser, HBOT, LLLT) is most effective, what’s evidence-based versus marketing-driven—these details determine whether a scar fades to a fine line or stays prominent. The standard discharge handout doesn’t get into it.
The full scar maturation framework and intervention timing—what works at week 6 versus month 6—is detailed in our scar care protocol guide.
Recovery mindset: The early phase of diastasis recti repair surgery recovery is about protecting the repair. The later phase is about rebuilding strength with correct pressure management—so the result lasts.
Safety, Surgeon Selection, and How to Reduce the Risk of a “Botched” Outcome
Because surgery to repair diastasis recti can be performed as a standalone repair or combined with contour procedures, outcomes vary based on planning, technique, and aftercare. Your goal isn’t just “a flatter abdomen”—it’s a safe repair that aligns with your anatomy and expectations. This is where an “expert patient” approach pays off: verify credentials, insist on clarity, and use medical science—not hype—to evaluate claims.
Key safety checkpoints: facility standards, anesthesia planning, and aftercare
Safety starts with fundamentals: an appropriately accredited surgical facility, a clear anesthesia plan tailored to your health status, and structured follow-up. If you’re traveling, aftercare logistics are not a detail—they’re part of the safety plan. Ask who you contact after hours, how early complications are handled, and what the plan is for follow-up visits.
“Verify credentials” is the line every patient nods at and almost no one actually executes. The verification process needs structure: which board certifications matter for diastasis-specific repair, how to confirm fellowship pedigree in abdominal wall reconstruction, why a plastic surgeon’s volume in this exact procedure matters more than total operating years, and which red flags surface only in surgeon-of-record contracts. Generic credential checks miss most of this.
The full credential-verification framework, including the surgeon-specific questions that protect against common gaps, is in our surgeon evaluation guide.
Facility evaluation for abdominal wall surgery has different priorities than facility evaluation for face or body contouring. The infrastructure that matters here includes mesh sterilization protocols when reinforcement is used, hernia-emergency response capacity, post-op fluid management for combined procedures, and the surgical-volume threshold below which a facility shouldn’t be performing combined repairs at all. International patients add a layer: aftercare continuity once you fly home matters more than amenities while you’re there.
The full accreditation criteria, infrastructure benchmarks, and the procedure-category-specific requirements that separate genuine surgical facilities from cosmetic-grade clinics are in our facility evaluation guide.
Mesh vs no mesh: questions grounded in scientific evidence
If your surgeon mentions reinforcement, make sure the “why” is specific to your case (e.g., hernia, tissue quality, recurrence risk). Recent evidence reviews and trials continue to compare mesh-supported approaches versus suture plication alone, with ongoing debate and the need for longer-term data in some subgroups—exactly the kind of nuance you should expect in a science-based discussion.
Here’s where the mesh-versus-suture conversation needs current evidence rather than dated assumptions. A 2025 systematic review and meta-analysis published in Surgical Endoscopy evaluated short-term outcomes for minimally invasive endoscopic onlay repair (ENDOR)—a mesh-supported technique gaining traction for combined diastasis-and-hernia presentations. The findings frame what’s actually known about perioperative safety and short-term outcome data: useful, but with the explicit caveat that long-term durability evidence still has gaps the field hasn’t filled.
The full endoscopic repair meta-analysis is the strongest current synthesis if you want the science behind newer mesh-supported approaches—useful when you want the evidence base, not just the surgeon’s preference.
How to interpret “diastasis recti repair surgery before and after” photos responsibly
Diastasis recti repair surgery before and after galleries can be useful, but only when they’re transparent and comparable. Photos are most reliable when they show:
- Similar posture (no “sucking in” or pelvic tilt tricks)
- Similar lighting and camera distance
- Clear time stamps (e.g., 6 weeks vs 6 months can look very different)
- Comparable anatomy (skin laxity, weight changes, whether lipo or tummy tuck was included)
The four-criterion photo audit is the bare minimum, not a finish line. A serious comparison needs sample size—dozens of cases across body types, ages, and procedure combinations—to spot the consistency patterns that distinguish a clinic’s actual outcomes from its marketing highlights. Single dramatic photos prove nothing; consistent patterns across many cases prove a lot.
The full transformation results gallery shows the range across our patient population, including the variations that surface when you audit beyond a curated handful.
Also ask what procedures were performed in each case. A dramatic “after” often reflects a combination approach, not just diastasis recti muscle repair surgery alone.
Consultation questions that protect you (technique, complications, revisions)
Bring these questions to any consultation for diastasis recti surgery repair:
- Is my plan a standalone repair, a tummy tuck + repair, or hernia repair + diastasis repair?
- How do you decide between plication-only vs reinforcement?
- What are the most common complications in your practice (seroma, wound issues, recurrence), and how are they managed?
- What does my diastasis recti repair surgery recovery plan look like week by week—especially lifting restrictions?
- If revision is needed, what is your policy and typical approach?
One question most consultations don’t include—even though it’s the single highest-leverage protection for international patients. “Will you personally perform every step of this surgery, and if not, who will, and is that documented in the consent?” Ghost surgery is the structural risk that pricing transparency, package quality, and even credential verification cannot solve. It only fails through contractual accountability, not technology.
The contractual clauses, identity-verification protocols, and the consent language that closes this loophole are mapped in our operating-room accountability protocol.
Frequently Asked Questions (FAQ): Diastasis Recti Repair Surgery
This FAQ answers the most common “expert patient” questions about diastasis recti repair surgery—including symptoms, recurrence, mesh, pregnancy planning, and what to expect during diastasis recti repair surgery recovery. Keep in mind: the best answer for you depends on whether your case is a standalone repair, part of a tummy tuck, and/or combined with hernia repair. When in doubt, bring these questions to your consultation and ask for case-specific reasoning supported by scientific research and clinical experience.
Can diastasis recti cause back pain and pelvic floor symptoms?
It can be associated with back discomfort and a feeling of core instability in some patients, especially during lifting or exercise, because the abdominal wall contributes to pressure management and trunk support. However, back pain and pelvic floor symptoms have many causes. A proper evaluation should consider posture, hip mechanics, pelvic floor function, and rule out hernias or other abdominal wall issues. This is why “treating the gap” alone isn’t always the full solution.
Will diastasis recti come back after surgery?
Recurrence is possible, but risk can be reduced with the right technique selection, weight stability, and a staged return to activity that respects lifting limits. Future pregnancy and significant weight fluctuations are two of the most common factors that can re-stretch the midline. Your surgeon should explain your personal recurrence risk based on tissue quality, the presence of a hernia, and the repair method used.
Is mesh always necessary?
No. Many cases of diastasis recti muscle repair surgery are performed with suture plication alone. Mesh may be considered when there is a concurrent hernia, poor tissue quality, or when reinforcement is judged to reduce recurrence risk. The key is individualized justification: you should understand why mesh is recommended, where it would be placed, and what trade-offs exist.
Can I get pregnant after diastasis recti surgery repair?
Many patients can become pregnant after diastasis recti surgery repair, but pregnancy can stretch the repair and affect results. If you are planning future pregnancies soon, many surgeons recommend postponing surgery when feasible—unless symptoms are severe or a hernia requires repair. If pregnancy is possible in the future, ask about timing, durability expectations, and what you can do to protect the repair.
How long before I can lift my child or return to the gym?
This is one of the most important recovery questions. Early lifting restrictions are common after surgery to repair diastasis recti, because straining can stress the repair before it stabilizes. Many protocols allow gradual activity progression over weeks, with heavier lifting and more intense exercise typically delayed until clearance—often around 6–8 weeks or longer depending on complexity and whether a tummy tuck/hernia repair was involved. Always follow your surgeon’s exact plan.
"Don't lift your child" sounds clinical until it's your reality at week 2. The actual logistics—who picks up the toddler, how the bath routine adapts, what positions actually protect the repair, when partner/family support windows need to overlap—are practical questions that determine whether the recovery plan survives contact with daily life. Most surgeon handouts skip this layer entirely.
The day-by-day postpartum recovery logistics, including the household adaptations that actually work, are mapped in our postpartum recovery practical guide.
What’s the difference between a mini tummy tuck and full tummy tuck for diastasis?
A mini tummy tuck generally addresses limited lower-abdominal skin laxity and may allow a more limited repair, whereas a full tummy tuck typically addresses more extensive skin laxity and often provides broader access to correct midline laxity along a longer segment. If your concern includes upper abdominal bulging and significant laxity above the navel, a full approach may be more predictable. Your anatomy—not the label—should decide the plan.
The mini-versus-full distinction comes up in almost every diastasis consultation, but the answer is rarely binary. Anatomy, diastasis length, skin laxity above and below the navel, scar preferences, and recovery tolerance all influence the decision. Choosing between them based on a label rather than anatomy is one of the more common drivers of "I should have done the other one" regret.
The full mini-versus-full breakdown, including which anatomy patterns favor each option, is in our tummy tuck scope comparison.
How do I know if I also have a hernia—and does that change the surgery?
A hernia can present as a focal bulge (often at or near the navel) that may worsen with coughing or straining. Sometimes it’s subtle and needs ultrasound or CT for confirmation. If a hernia is present, the operation may become “hernia repair + diastasis repair,” and this can change technique decisions (including whether reinforcement is considered), recovery restrictions, and sometimes diastasis recti repair surgery cost.
Why do some people still have a “pooch” even after repair?
Because not all abdominal contour is caused by diastasis. Loose skin, fat distribution, posture (e.g., anterior pelvic tilt), and overall core control can all contribute. That’s why diastasis recti repair surgery before and after results look dramatically different depending on whether a tummy tuck and/or liposuction was included—and why honest surgeons separate “structural repair” from “skin and contour” goals.
Is there a “best” technique for repair diastasis recti surgery?
There isn’t one best method for everyone. The best technique is the one matched to your anatomy (severity, tissue quality, presence of hernia, skin excess), goals (functional vs cosmetic), and risk profile. A science-based consultation should clearly explain the rationale for technique selection and what outcomes are realistic.
What should I bring to my consultation to get the most accurate plan?
Bring: (1) your symptom list and activity limitations, (2) your medical/surgical history, (3) your rehab history (what you tried and for how long), (4) questions about diastasis recti repair surgery recovery and restrictions, and (5) a clear list of goals (function, contour, or both). If you’re comparing clinics, insist on a line-item quote so you can interpret diastasis recti repair surgery cost accurately (what is included vs excluded).
Medical Disclaimer: This page is provided for general educational purposes only and does not replace a face-to-face medical consultation, diagnosis, or personalized treatment plan. All surgery carries risks and outcomes vary between individuals. Suitability for a diastasis recti repair, procedure selection, and anesthesia choice can only be determined after a full clinical assessment by a qualified surgeon. Always follow your clinician’s instructions and seek urgent medical attention if you develop concerning symptoms during recovery.










