If you’re researching a facelift, one metric keeps coming up for “safety” and predictability: facelift revision rate. On paper it sounds simple—how often a patient needs another operation. In real life, it’s a nuanced outcome measure influenced by technique, patient selection, follow-up length, and even how a clinic defines the word “revision.”
This article is written for the expert patient mindset: you want the why, not slogans. We’ll use a medical science lens—how surgical experience changes decision-making, how complications are prevented, and how you can evaluate claims using scientific research-style questions rather than marketing language.



What you’ll be able to do after reading:
- Understand what a facelift revision rate actually measures (and what it hides).
- See why “expert vs novice” is less about years alone and more about judgment under complexity.
- Ask consultation questions that surface real-world revision risk—especially if you’re considering medical travel or a revision facelift Turkey option.
Key takeaway: A lower revision rate is meaningful only when you know how it was defined, who was included, and how long outcomes were tracked.
| Term You’ll Hear | What It Usually Means | Why It Can Confuse Patients |
|---|---|---|
| Revision | A second operation to correct an aesthetic or medical problem after healing | Some clinics count only “major” revisions; others include minor scar revisions |
| Touch-up | A small corrective procedure (sometimes under local anesthesia) | May be counted as a “revision” in one practice and not in another |
| Staged plan | A planned second step (e.g., later fat grafting) discussed upfront | Can look like a “revision” if the plan wasn’t clearly documented |
| Revision facelift surgery | A true secondary facelift performed to correct or refine a prior facelift | Often technically harder than a primary facelift; not all surgeons specialize in it |
Table of Contents

What Is a Facelift Revision Rate (and What It Doesn’t Tell You)
A facelift revision rate is the proportion of patients who undergo facelift revision surgery after their initial procedure—within a defined time period—because they need correction or improvement. The problem is that many public-facing “rates” don’t state (1) the time window, (2) what counts as a revision, and (3) how complex the starting cases were. Without those details, you can’t compare surgeons fairly—especially when evaluating a primary surgeon versus a specialist in revision facelift work.
A clear definition: numerator, denominator, and time window
To evaluate any quoted revision rate, you need three elements:
- Numerator: How many patients had a second operation?
- Denominator: Out of how many facelift patients total?
- Time window: Was it tracked for 6 months, 1 year, 3 years, or longer?
Longer follow-up often reveals more late issues (scar maturation, contour irregularities, recurrent laxity). A surgeon who tracks outcomes for years may appear to have a “higher” rate simply because they measure more honestly.
True revisions vs planned touch-ups vs staged procedures
A true revision is typically performed because something went wrong medically (e.g., significant scar problems) or aesthetically (e.g., distortion, marked asymmetry, unnatural tension effects). A “touch-up” may be minor and sometimes office-based. A staged plan can be part of sound strategy—especially in older patients or those with thin skin—yet can be misread as “failure” if the plan isn’t transparent.
For the expert patient, the most important question is: Was the second step planned from the beginning, or was it required to fix a problem?
Why reported rates vary (case-mix, follow-up duration, reporting bias)
Rates vary because not all practices treat the same patient population. Surgeons who accept high-risk cases—smokers, patients after massive weight loss, patients with prior facelifts, or complex anatomy—may see more revision work. Some clinics also attract patients seeking revision facelift surgery specifically, which naturally increases their “revision” volume, but that may reflect expertise rather than poor outcomes.
Finally, reporting bias matters: marketing pages tend to simplify. A more scientific research approach is to ask for the definition, timeframe, and case-mix so you can interpret the number responsibly.
Benchmarks: What “Normal” Looks Like in Modern Facelift Surgery
Patients often ask for a single “normal” number. In reality, benchmarks depend on technique (mini lift vs SMAS vs deep plane), patient factors, and whether the surgeon is performing mostly primary cases or doing complex revision facelift corrections referred from elsewhere. So instead of anchoring on one percentage, use benchmarks as a framework for questions: What does this surgeon consider a revision? How are complications handled? What is their protocol if healing doesn’t go as planned?
Where benchmarks come from (peer-reviewed data vs marketing claims)
In medical science, meaningful benchmarks come from peer-reviewed studies with clear definitions and consistent follow-up. Marketing claims often lack that structure. If a clinic cites a rate, ask for: (1) the follow-up duration, (2) whether revisions include minor scar corrections, and (3) whether the dataset includes revision facelift surgery patients coming in after other surgeons.
How technique affects expectations (mini, SMAS, deep plane)
Technique influences both durability and the type of issues that might lead to revision. A limited/mini lift may be appropriate for mild laxity but can under-correct more advanced aging, creating “I need more” dissatisfaction rather than a true surgical complication. More structural approaches (e.g., deep plane) can create longer-lasting midface/neck improvement in selected patients, but they demand high-level anatomical skill and consistent intraoperative judgment—areas where experience tends to matter most.
Patient factors that change revision likelihood (smoking, weight changes, skin quality)
Even with an expert surgeon, patient factors heavily influence revision risk. Smoking/nicotine exposure affects microcirculation and wound healing. Major weight changes can alter facial volume and laxity. Skin quality (sun damage, thin dermis, prior aggressive resurfacing) can increase scarring or irregularities. These are also common primary facelift failure causes when they aren’t identified and counseled properly preoperatively.
If you are traveling for care (including revision facelift Turkey pathways), it’s even more important that your surgeon documents these risks clearly and has a structured follow-up plan across borders.
Why Expert Surgeons Typically Have Lower Revision Rates
When patients compare “expert vs novice,” they often focus on years in practice. But revision outcomes are driven less by a calendar and more by repeatable decision-making under complexity: choosing the right technique for the right anatomy, avoiding tension-related distortions, controlling bleeding, and managing tissue health so healing is predictable. In many cases, what patients call a “failed facelift” is actually a chain of small decisions that compound—this is where experience most often shows up in the facelift revision rate.
Volume + specialization: what experience really changes
In surgery, repetition doesn’t just make you faster—it makes your “pattern recognition” sharper. Expert surgeons tend to:
- Anticipate risk (who is likely to bruise, swell, scar poorly, or heal slowly).
- Standardize steps that reduce avoidable variability (incision planning, tension vectors, closure technique).
- Detect problems early and intervene before they become revision-level issues.
This matters even more in revision facelift surgery, where tissues may be scarred, blood supply can be compromised, and anatomy is less “textbook.” A surgeon who routinely handles complex cases usually develops safer strategies for those realities.


Anatomy-first technique selection (when deep plane matters)
A key difference between expert and novice behavior is technique selection. Novices may default to what they do most often—even if your anatomy calls for something else. Experts are more likely to ask:
- Is the laxity primarily skin-level, or is there deeper structural descent?
- Is the neck the main issue (platysma bands, submental fullness), and does it require a dedicated plan?
- Will a limited lift under-correct and create “I still look tired” dissatisfaction?
Under-correction is one of the under-discussed primary facelift failure causes. It doesn’t always look like a “botched” result—sometimes it simply fails to deliver a meaningful change, leading patients to seek a revision facelift sooner than expected.
Intraoperative judgement: tension vectors, hemostasis, symmetry control
Many revision triggers are not dramatic events—they’re subtle issues that become obvious over time. Experts generally put more emphasis on:
- Natural tension vectors: avoiding an overpulled appearance and preventing earlobe distortion (the “pixie ear” effect).
- Hemostasis (bleeding control): reducing hematoma risk, which can directly increase complication-related revisions.
- Symmetry discipline: checking neck/jawline balance repeatedly before closure.
From a medical science perspective, these are “process controls.” They lower the probability of complications that later require facelift revision surgery.
| Factor | More Typical of Expert Surgeons | More Typical of Novice Surgeons |
|---|---|---|
| Case selection | Clear inclusion/exclusion criteria; realistic counseling on limits | Broader inclusion; higher chance of taking mismatched candidates |
| Technique match | Anatomy-driven choice; plans the neck and midface deliberately | Technique-driven choice; may “fit” the patient into the technique |
| Tension management | Prioritizes structural support over skin pull | Higher risk of skin-tension outcomes (distortion, widened scars) |
| Complication response | Defined pathway for swelling/hematoma/scar problems | More reactive; higher chance minor issues progress |
| Revision readiness | Comfortable with secondary anatomy; plans staged solutions if needed | Less experienced with scarred planes and altered blood supply |
Practical interpretation: If you want to compare revision risk fairly, ask surgeons how they define “revision,” what their follow-up window is, and what portion of their work is primary vs revision facelift surgery.
Where Novice Surgeons Are More Likely to Run Into Problems
It’s important to say this carefully: every surgeon starts somewhere, and a “novice” label doesn’t automatically mean unsafe. The risk comes from predictable failure points—especially when a procedure is treated as “mostly skin tightening,” or when planning and aftercare systems are thin. These are the scenarios that can raise the chance of a later revision facelift consult, including among patients who travel for care (for example, those researching revision facelift Turkey as a solution after an unsatisfactory first surgery elsewhere).
Common technical errors (wrong plane, over-tightening, poor structural handling)
Common technical issues that can increase revision likelihood include:
- Operating in the wrong tissue plane: can lead to insufficient lift, contour irregularities, or prolonged swelling.
- Over-reliance on skin tension: increases risk of an unnatural “pulled” look and widened scars.
- Inconsistent neck strategy: under-addressing platysma bands or submental laxity can make results look incomplete.
These problems often show up as “it looked okay early, then it didn’t age well,” which is a classic path toward revision facelift surgery.
Planning gaps (candidate selection, unrealistic goals, weak risk counseling)
Many primary facelift failures start before the first incision. Planning gaps include:
- Not screening nicotine exposure properly (including vaping and patches), increasing wound-healing risk.
- Not aligning goals with anatomy (expecting midface change from a limited approach).
- Under-explaining normal healing, leading patients to chase “early revision” during the swelling phase.
From a scientific research mindset, think of this as “input quality.” Poor inputs create poor outputs—even if the surgery itself is technically competent.
Systems issues (team consistency, anesthesia plan, postop protocols)
A facelift is not only the surgeon’s hands—it’s also the system around the patient. Novice environments may have:
- Less standardized postop monitoring for bruising, hematoma signs, or early skin compromise.
- Inconsistent wound/scar protocols, which affects visible outcomes.
- Weaker continuity of care, especially for international patients who need structured remote follow-up.
These system-level gaps can turn manageable issues into revision-level problems—one reason expert patients often ask not only “who is the surgeon?” but also “what is the clinic’s pathway if recovery deviates from the ideal?”
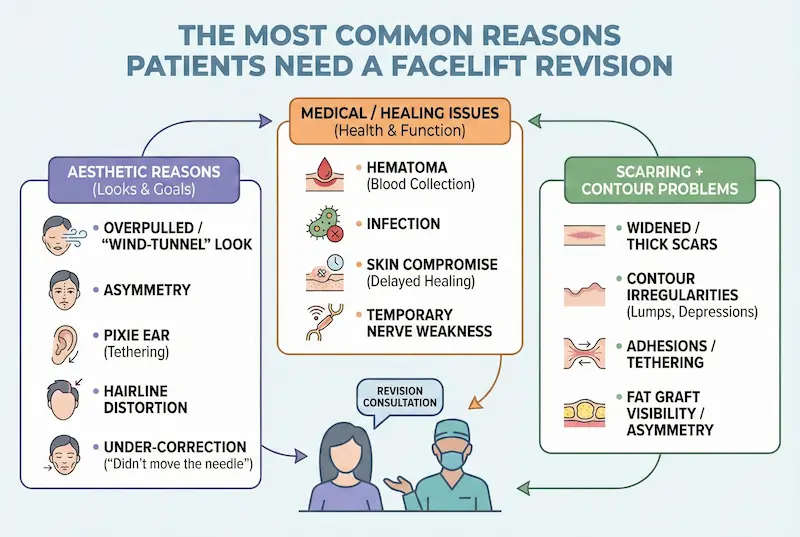
The Most Common Reasons Patients Need a Facelift Revision
Most patients imagine revision as a dramatic “botched” scenario. In practice, the reasons for revision facelift surgery fall into two broad buckets: (1) aesthetic outcomes that don’t match the patient’s goals or look unnatural, and (2) medical/healing issues that create visible problems (scars, contour defects) or functional concerns. Understanding these categories helps you interpret facelift revision rate more intelligently—and spot the primary facelift failure causes during consultations.
Aesthetic issues (overpulled look, asymmetry, pixie ear, hairline distortion)
Aesthetic-driven revisions are often about tension, vectors, and planning—not simply “tightening more.” Common triggers for a revision facelift consultation include:
- Overpulled / “wind-tunnel” look: typically linked to skin-based tension rather than structural support.
- Asymmetry: may reflect natural baseline asymmetry amplified by uneven lift vectors or swelling patterns.
- Pixie ear (earlobe tethering): often tension-related; can worsen with time.
- Hairline distortion: temporal hairline shifting or visible incision issues, especially if incision placement and closure aren’t meticulous.
- Under-correction: the facelift “didn’t move the needle,” which is a frequent, quiet primary facelift failure cause (wrong procedure for the degree of laxity).
Medical/functional issues (hematoma, infection, skin compromise, nerve weakness)
Medical complications are less common but more urgent when they occur—and they can increase the likelihood of later facelift revision surgery. The most important ones include:
- Hematoma: a significant collection of blood under the skin; can compromise skin health and increase scarring risk if not treated promptly.
- Infection: can threaten wound healing and scar quality.
- Skin compromise (delayed healing / tissue survival problems): more likely in smokers, patients with vascular issues, or overly aggressive tension/undermining.
- Temporary nerve weakness: often resolves, but persistent issues may require expert evaluation.
Expert-patient note: A clinic’s “revision rate” matters less than its complication pathway—what happens on day 1, day 3, and week 2 if recovery deviates from the ideal.
Scarring + contour problems (irregularities, adhesions, fat graft issues)
Many revisions are scar/contour-focused rather than full “redo” surgery. These can include:
- Widened or thick scars: influenced by incision design, closure technique, patient biology, and aftercare.
- Contour irregularities: lumps, depressions, or edge lines—sometimes from uneven tissue handling or fluid collections.
- Adhesions / tethering: scar tissue can pull the skin in unwanted directions, especially after prior surgery.
- Fat graft visibility or asymmetry: when fat survival is uneven or placed too superficially.
| Revision Driver | How It Typically Presents | Common “Root Cause” Pattern | How Experts Try to Prevent It |
|---|---|---|---|
| Overpulled look | Unnatural tightness, lateral pull | Skin-tension strategy | Structural support + correct vectors |
| Pixie ear | Earlobe tethering, downward pull | Excess tension near ear closure | Tension distribution + earlobe positioning |
| Under-correction | “Not enough change” | Wrong procedure for anatomy | Anatomy-driven technique selection |
| Hematoma | Rapid swelling, pain, bruising | Bleeding control / postop monitoring | Hemostasis discipline + early detection pathway |
| Scar/contour issues | Visible scars, lumps, tethering | Closure quality + patient biology + aftercare | Meticulous closure + structured scar protocol |
How a Specialist Approaches Revision Facelift Surgery (Why It’s Not “Just Another Facelift”)
Revision facelift surgery is often more technically demanding than a primary facelift because the surgeon is working with altered anatomy: scar tissue, less predictable blood supply, and sometimes distorted landmarks. This is why comparing “revision capability” is crucial if you suspect you may need a revision facelift—or if you’re exploring options such as revision facelift Turkey after an unsatisfactory first procedure elsewhere.
Scar tissue changes the surgical “map”
Scar tissue can bind planes together and make dissection more difficult. It also changes how skin and deeper tissues move. A revision specialist typically plans more conservatively, prioritizing tissue safety and blood supply before chasing maximal tightening.
Blood supply and tissue survival matter more than “tightness”
When tissue has been lifted before, blood flow patterns can be less robust. This is why risk factors like nicotine exposure become even more critical in revisions. An expert revision approach often focuses on safe repositioning and strategic support rather than aggressive tension.
Patient Reality Check: What “Success” Feels Like (Not Just How It Photographs)
Expert patients often look for consistency: natural expression, minimal pain, and results that don’t announce “surgery.” In AKM Clinic’s patient testimonials, several facelift patients describe outcomes in those terms. For example, Barbara (USA) wanted a natural change—she described looking like “nothing happened but probably 20 years younger.” Sarah emphasized feeling “refreshed” and “over the moon” months later. While individual experiences are not scientific proof, they can help you understand what high-satisfaction outcomes sound like when patients talk about function, comfort, and naturalness—not just selfies.
How to Evaluate a Surgeon’s Real-World Revision Risk (Questions to Ask)
If you want a practical way to estimate your personal revision risk, treat the consultation like a mini scientific research interview. You’re not being “difficult”—you’re clarifying definitions, denominators, and systems. This approach is especially important if you are comparing multiple surgeons, or if you’re considering traveling for a revision facelift Turkey solution after an unsatisfactory first procedure.
The “revision rate” questions that reveal truth (definitions, tracking, timeframe)
- “How do you define a revision?” Ask whether they include scar revisions, ear corrections, hematoma-related re-operations, or only major secondary facelifts.
- “What follow-up window is your rate based on?” Six months and three years can look very different.
- “How many of your cases are primary vs revision facelift surgery?” A surgeon who accepts complex revision facelift referrals will have a different case-mix.
- “What are the top 3 primary facelift failure causes you see—and how do you prevent them?” The quality of this answer tells you more than a number.
How to read before-after photos like an expert (consistency + long-term follow-up)
Before-after photos can be informative, but only if you read them correctly:
- Look for consistency across many patients, not one “hero” result.
- Check neck and jawline continuity (not just the cheek area).
- Watch for tension signals: distorted earlobes, widened scars, hairline displacement, “pulled” corners of the mouth.
- Ask for longer-term examples (e.g., 6–12 months), because early swelling can hide issues.
Safety signals (facility standards, emergency readiness, complication pathway)
Revision risk is tightly linked to safety systems. Ask how the clinic handles:
- After-hours swelling/hematoma concerns (who answers, what happens next).
- Documented postop checkpoints (day 1–3 monitoring matters).
- Clear escalation pathways for wound issues or skin compromise.
Expert-patient filter: A surgeon who can explain their complication pathway calmly and precisely is usually operating with mature systems.
| Question You Ask | Reassuring Answer Sounds Like | Concerning Answer Sounds Like |
|---|---|---|
| “What counts as a revision?” | Clear definition + examples + timeframe | Vague, defensive, or purely marketing language |
| “How do you prevent primary facelift failure causes?” | Specific: candidate selection, technique match, tension strategy, aftercare protocol | “It never happens” / “We’re the best” without process detail |
| “What happens if recovery deviates?” | Step-by-step monitoring + escalation plan | No clear pathway or shifts responsibility to the patient |
Red Flags and Smart Safeguards for the “Expert Patient”
Many revision journeys start with a preventable mismatch: wrong procedure, rushed planning, or unrealistic expectations. Below are safeguards that reduce your chance of needing facelift revision surgery—and they matter whether you’re doing a primary operation or considering a revision facelift after a prior surgery.
Marketing vs evidence: spotting exaggerated claims
- Red flag: “Zero complications” or “0% revision rate.” In real medical science, honest systems acknowledge risk and explain mitigation.
- Safeguard: Ask for definitions, follow-up windows, and what they do when healing is not ideal.
- Red flag: One-size-fits-all technique offered to every patient.
- Safeguard: Look for anatomy-driven planning and clear rationale.
Consultation quality checklist (exam depth, plan logic, risk transparency)
A high-quality consultation usually includes:
- A structured facial assessment (midface, jawline, neck, skin quality, and asymmetry).
- Technique reasoning (why this approach fits your anatomy and goals).
- Risk counseling tailored to you (nicotine exposure, prior scars, medication, bleeding risk).
- Clear recovery timeline including what is normal vs not normal.
Medical tourism safeguards (continuity of care, follow-up structure, documentation)
If you’re traveling—especially for complex work like revision facelift Turkey—continuity matters:
- Get your operative notes and a written procedure summary.
- Confirm a remote follow-up schedule (video calls, photo checkpoints, messaging access).
- Clarify who manages issues after you return home and how the clinic coordinates care if needed.

Recovery and Aftercare Factors That Influence Revisions
Some patients pursue revision facelift options too early—when they’re still in the normal swelling and scar-maturation window. Others develop avoidable scar or contour problems due to inconsistent aftercare. The point is not to chase “perfection fast,” but to support biology so results settle naturally and predictably.
Timeline realities: swelling vs scar maturation vs “too-early revision”
Most facelift concerns fall into three timing categories:
- Early (days to weeks): swelling, bruising, tightness, unevenness—often normal and improving.
- Mid (weeks to months): scar remodeling and contour settling; some asymmetry can persist temporarily.
- Late (months to 1+ year): scar maturation completes and true “final” contours are clearer.
Many expert surgeons prefer waiting before labeling something as a revision-worthy problem—unless there is a medical complication that needs immediate action.
Healing support that can reduce complications (HBOT + LLLT as adjuncts)
In AKM Clinic’s patient care standards, two supportive technologies are highlighted as recovery adjuncts: Hyperbaric Oxygen Therapy (HBOT) and Low-Level Laser Therapy (LLLT). These tools are described as being used to support healing biology—an approach consistent with the “process control” thinking you see in scientific research culture.
- HBOT (Hyperbaric Oxygen Therapy): presented as supporting tissue survival and regeneration by increasing oxygen availability, and described as supporting scar healing and reducing postoperative inflammation/swelling.
- LLLT (Low-Level Laser Therapy): described as supporting recovery through mechanisms such as enhanced collagen synthesis and reduced inflammation, while being non-thermal (no damaging heat) in principle.
Important nuance: Adjunct technologies can support recovery, but they don’t replace surgical planning, safe technique, and good aftercare. Think “risk reduction,” not “guarantee.”
When revision is appropriate—and when waiting is safer
Consider evaluation for revision facelift surgery when:
- A clear tension distortion is present (e.g., worsening pixie ear),
- There are persistent contour defects after appropriate healing time,
- Scars mature poorly despite structured scar care,
- Or there is a true complication that requires surgical correction.
Waiting is often safer when the issue is early swelling, temporary tightness, or scar immaturity.
Frequently Asked Questions (FAQ): Facelift Revision Rate
Below are concise answers to common expert-patient questions about facelift revision rate, facelift revision surgery, and decision-making around a revision facelift pathway.
What is a “good” facelift revision rate?
There isn’t one universal “good” number without context. A meaningful comparison requires the same definition of “revision,” similar case complexity, and a similar follow-up window.
How long should you wait before considering a revision?
Many surgeons prefer waiting months for swelling to resolve and scars to mature—unless there’s a medical issue (e.g., hematoma) that requires urgent intervention. Timing should be individualized.
Are mini facelifts more likely to need revision than deep plane facelifts?
Not always. Mini lifts can be appropriate for mild laxity. Revisions become more likely when the chosen procedure under-corrects the true anatomic problem—one of the more common primary facelift failure causes.
Do age and skin quality significantly affect revision risk?
Yes. Skin quality, sun damage, and healing biology can influence scarring and contour settling. Age alone isn’t the only factor—tissue quality and overall health matter more.
Can a facelift be revised more than once?
Yes, but each surgery can increase scarring and complexity. This is why choosing a surgeon with strong planning and revision capability is important from the start.
Which complications most commonly lead to revision surgery?
Revision triggers include tension-related distortions, significant asymmetry, problematic scars, contour irregularities, and complication-related issues such as hematoma consequences or delayed healing.
How can I verify a surgeon’s experience and outcomes?
Ask for long-term follow-up examples, a clear definition of revisions, the timeframe used for tracking, and how many cases are primary versus revision facelift surgery. Evaluate the consultation depth and the clinic’s complication pathway.
If you’d like to go beyond facelift revision rate and explore related safety and decision-making topics, you can also review our guides on Best Deep Plane Facelift Clinic in Turkey, Plastic Surgeon Board Certification, and Questions to Ask Plastic Surgeon to strengthen your surgeon-selection checklist. For added peace of mind, we also recommend reading about Ghost Surgery in Turkey and how to avoid it, plus practical tips in English Speaking Plastic Surgeons in Turkey for clear communication during consultations. And if your concerns involve scars after a prior procedure, you may find Scar Revision Surgery Turkey helpful as a next step.
Medical Disclaimer: This page is provided for general educational purposes only and does not replace a face-to-face medical consultation, diagnosis, or personalised treatment plan. All surgery carries risks and outcomes vary between individuals. Suitability for a facelift surgery, procedure selection, and anaesthesia choice can only be determined after a full clinical assessment by a qualified surgeon. Always follow your clinician’s instructions and seek urgent medical attention if you develop concerning symptoms during recovery.