





Butt implants (also called gluteal implants) are a surgical option for increasing buttock projection and improving shape when exercise, weight changes, or naturally limited fat volume can’t create the desired contour. Unlike fat transfer (BBL), which relies on your body’s own fat survival, implants use a pre-formed medical-grade device designed specifically for the gluteal region to provide predictable, structural volume.
This guide is written for the “expert patient”—someone who wants technical clarity, realistic expectations, and a transparent discussion of risks. You’ll learn what butt implants are made of, who tends to be a good candidate, how different placement planes change outcomes, what recovery actually feels like, and how to evaluate safety and surgeon qualifications.
Table of Contents
What Are Butt Implants?
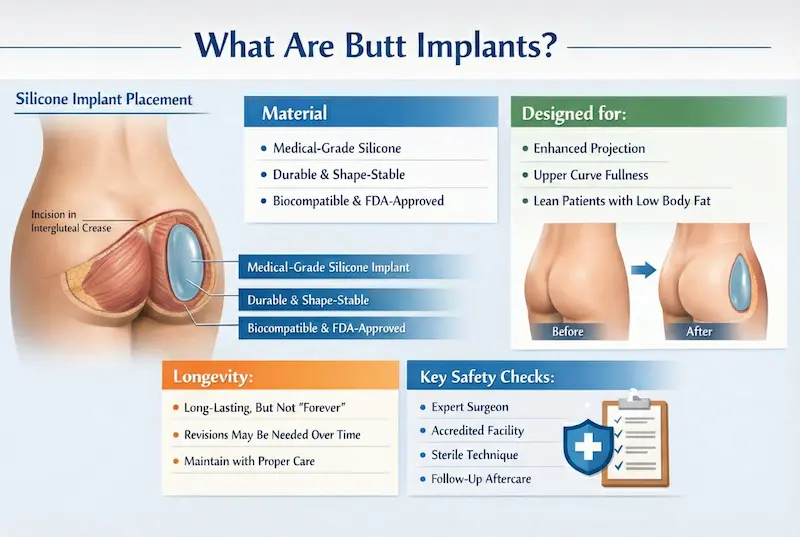
Butt implants are specialized silicone implants placed through a hidden incision (most commonly within the intergluteal crease) and positioned in a carefully created pocket to enhance size, projection, and contour. The “best” result is not the biggest result—it’s the one that matches your anatomy, skin quality, posture, and lifestyle with a stable implant plan and a recovery you can realistically follow.
What butt implants are made of
Most modern butt implants are made from medical-grade silicone elastomer engineered for the unique mechanical demands of the buttocks—pressure, movement, and sitting. Depending on the manufacturer and model, implants may be described as solid silicone or highly cohesive silicone. The key point is that gluteal implants are built to be more durable and shape-stable than many implants used in other areas of the body.
When evaluating implant materials, the expert patient should focus on:
- Biocompatibility: The material must be designed to live in the body long-term with a low inflammatory profile.
- Durability and tear resistance: The gluteal region experiences repetitive stress from motion and sitting.
- Shape stability: The implant should maintain projection and smooth contour without visible edges in motion.
- Quality and traceability: Reputable manufacturers provide documentation, batch tracking, and device labeling.
In the United States, many patients look specifically for FDA-approved implants when available for a given indication. In other settings, the principle is the same: choose a surgeon who can clearly explain the implant type, why it was selected for your anatomy, and what documentation is provided.
Who butt implants are designed for
Butt implants are not “one aesthetic.” They can be planned for different goals, such as:
- Projection: Creating a more pronounced outward curve, especially in patients with naturally flat buttocks.
- Upper-pole fullness: Improving roundness higher on the buttock when fat transfer isn’t feasible.
- Structural enhancement: Adding volume in a way that doesn’t depend on fat survival (important for very lean patients).
Implants can be particularly useful when a patient has:
- Low body fat (limited donor fat for BBL)
- Significant “flatness” with minimal projection despite training
- Desire for a predictable volume increase that does not fluctuate with weight changes as much as fat grafting can
That said, implants are not ideal for everyone. Skin quality, tissue thickness (coverage), sitting/athletic demands, and willingness to follow strict early recovery rules strongly influence candidacy and outcome.
How long butt implants can last
High-quality gluteal implants are designed for long-term durability, and many patients keep them for many years. However, it’s important to understand the difference between device durability and lifetime guarantee: no implant is “forever” in a way that eliminates the possibility of future surgery.
Reasons a patient might consider revision or replacement in the future can include:
- Capsular contracture: Scar tissue around the implant becomes tight or distorted (severity varies).
- Implant malposition: Shifting, asymmetry, or “edge visibility,” often related to pocket design, tissue coverage, or early strain.
- Patient preference changes: Desire for a different size/shape as body goals evolve.
- Weight and aging changes: The implant remains stable, but surrounding tissues change over time.
A realistic long-term mindset is: butt implants can be a durable solution, but they require proper plane selection, precise pocket control, and a surgeon who can explain how complications are prevented and managed if they occur.
Gluteal Anatomy & Aesthetic Planning
Excellent butt implant results come from anatomy-first planning. The gluteal area is dynamic: it moves when you walk, sits under constant mechanical stress, and changes with posture. A safe, natural-looking plan balances three variables—implant, tissues, and vector of movement—so the implant looks smooth not only standing still, but also in motion, consistent with core principles of medical science.
Key anatomy that influences implant planning
The buttock contour is shaped by several layers:
- Skin and dermis: Determines how well the surface can “drape” without rippling.
- Subcutaneous fat: Provides soft coverage and edge camouflage (thin patients have less).
- Fascial layer: A strong connective layer that can help support certain placement planes.
- Gluteus maximus muscle: A major structural component that affects pocket stability and movement dynamics.
Because the buttocks bear weight, the surgeon must plan for how tissues respond to pressure from sitting and how muscle contraction influences implant position. This is one reason plane choice (intramuscular vs subfascial, discussed later) is not a minor technical detail—it is central to stability and safety.
Defining goals: projection, shape, and “natural” balance
“Natural” is not a single look. For many patients, it means a buttock contour that matches body proportions—waist-to-hip relationship, thigh transition, and the hip dip area—without visible implant borders. Planning typically considers:
- Projection target: How far outward the buttock should extend relative to the lower back and thighs.
- Upper vs lower pole: Where fullness is needed to create a balanced silhouette.
- Lateral contour: How the side profile transitions into the hip and outer thigh.
- Symmetry: Natural asymmetry is normal, but the plan should minimize visible imbalance.
Surgeon’s Insight: The most convincing aesthetic surgery is the kind that doesn’t announce itself. The goal is rejuvenation, not alteration—enhancing your own proportions instead of forcing an artificial shape.
In practice, this means selecting an implant size and shape that your tissues can cover well, rather than “maxing out” volume beyond what your anatomy can support.
Female vs male butt implants: planning differences
While every plan is individualized, male and female aesthetic goals often differ in how projection and lateral fullness are balanced:
- Female planning: Often prioritizes a softer hourglass transition, with emphasis on roundness and upper-to-mid buttock fullness, while maintaining smooth blending into thighs.
- Male planning: Often aims for athletic projection and definition without exaggerated lateral width, maintaining a strong, proportionate frame.
- Coverage considerations: Leaner patients (common in male candidates) may have less fat coverage, making implant selection and plane strategy even more critical.
Regardless of gender, the best planning starts with an honest assessment of tissue thickness, skin elasticity, and lifestyle factors (sitting-heavy jobs, sports, and recovery compliance). These variables often matter more than the “ideal” look a patient brings from reference photos.
Ideal Candidates & Who Should Avoid Butt Implants
Butt implants can be an excellent option when you want a predictable increase in projection but don’t have enough donor fat for a BBL—or when you want structural enhancement that is less dependent on fat survival. The best candidates are those with realistic expectations, adequate tissue coverage, and the ability to follow strict early recovery rules (especially sitting and activity restrictions).
Candidate checklist (who tends to do well)
While candidacy is always individualized, patients who typically do best with butt implants often share these characteristics:
- Stable weight: Major weight fluctuations can change how surrounding tissues drape over the implant.
- Adequate soft-tissue coverage: Enough subcutaneous tissue to help camouflage implant edges and reduce visible “step-offs.”
- Good skin quality: Skin that can adapt to added volume without excessive laxity or distortion.
- Clear, anatomy-matched goals: Seeking proportionate projection rather than extreme size beyond tissue capacity.
- Strong recovery compliance: Willingness to avoid pressure on the area, follow garment/drain instructions if used, and respect activity limits.
During consultation, the most important questions are not “What size can I get?” but:
- How much coverage do I have for smooth edges?
- Which placement plane offers the best stability for my anatomy and lifestyle?
- What restrictions can I realistically follow during the first 2–6 weeks?
When a BBL may be better than implants (and when implants may be better)
Butt implants vs BBL is not just a cosmetic comparison—it’s a comparison of biology and anatomy. A BBL (fat transfer) can be a great option when you have adequate donor fat and want smoother overall contouring (including hips/waist shaping) with “tissue-like” softness. However, fat survival varies, and results can change with weight fluctuations.
Implants may be a stronger fit when:
- You are lean with limited donor fat for meaningful augmentation.
- You want a more predictable projection increase that doesn’t depend on fat take.
- Your goal is structural fullness rather than generalized contouring.
BBL may be a better fit when:
- You want broader contouring (waist-to-hip shaping), not just projection.
- You have sufficient donor fat and accept that some resorption is normal.
- You prefer avoiding an implant device and understand the trade-offs.
Some patients benefit from a hybrid approach (implant for projection + conservative fat grafting for edge blending), but the decision depends on tissue thickness, goals, and risk profile. This is discussed in detail in the “Butt Implants vs BBL” section later in this guide.
Pre-op screening and who should avoid butt implants
Safety starts long before the operating room. A responsible plan includes a thorough medical history, physical exam, and risk assessment—especially for infection risk, wound healing issues, and anesthesia considerations. Patients may be advised to postpone or avoid butt implants if they have:
- Uncontrolled diabetes or conditions that significantly impair wound healing
- Active smoking or nicotine use (nicotine strongly increases wound complications)
- Significant immune compromise or recurrent infection issues
- Severe skin laxity where added volume won’t address the primary concern
- Inability to follow recovery restrictions (work/lifestyle that forces early sitting or strenuous activity)
For expert patients, the “green flag” is a clinic that insists on candidacy standards rather than pushing everyone into surgery. For example, AKM Clinic explicitly frames safety around strict pre-operative health screenings to confirm candidacy before proceeding.

Types of Butt Implants, Shapes & Sizes
Modern gluteal implants come in different shapes, sizes, and profiles. The goal is not to chase a trend—it is to choose an implant that your tissues can cover smoothly, that matches your pelvic and gluteal anatomy, and that can be placed in a stable pocket with a low risk of edge visibility or shifting.
Implant shapes (round vs anatomic) and what they change
In broad terms, butt implants are designed to create either more generalized roundness or a more anatomically distributed projection. The “right” shape depends on where you need fullness and how your tissues distribute volume.
| Implant Concept | Typical Visual Effect | Who it may suit | Key planning considerations |
|---|---|---|---|
| Round / higher-profile concepts | More pronounced projection; can add “pop” to the buttock | Patients prioritizing projection with adequate tissue coverage | Avoid oversizing to reduce edge visibility and malposition risk |
| Anatomic / oval concepts | More distributed fullness; potentially smoother transition | Patients seeking softer contouring or specific directional fullness | Precise pocket orientation matters for symmetry and stability |
Regardless of the label, what matters most is how the implant behaves in your body: stability in motion, smooth edges, and proportionate contour from multiple angles.
Butt implant sizes and how sizing is chosen
Size selection is one of the most common areas where expert patients want clarity. The safest sizing process is anatomy-based and includes:
- Tissue coverage assessment: Thinner patients generally need more conservative sizing to maintain smooth edges.
- Pelvic width and gluteal footprint: The implant must “fit” the underlying anatomy without forcing lateral distortion.
- Skin elasticity: Tight skin may tolerate less volume, while lax skin may need a different strategy (sometimes not implants alone).
- Lifestyle factors: Sitting-heavy routines and high-impact sports can influence plane choice and conservative sizing decisions.
For patients who want a highly visual planning process, pre-operative simulation can be useful to align expectations. AKM Clinic notes its investment in 3D Vectra imaging for meticulous planning and surgical simulation, which can help patients understand realistic outcomes before committing to a plan.
Pocket planning, symmetry, and “natural edge” control
Two patients can receive the same implant size and look completely different—because the result depends heavily on pocket design and symmetry control. A well-designed pocket should:
- Hold the implant securely to reduce shifting, rotation, and asymmetry.
- Respect natural landmarks so the implant blends smoothly into upper and lower buttock contours.
- Minimize visible edges by balancing implant width, profile, and tissue coverage.
Because natural asymmetry is common, planning should also include a clear conversation about what “symmetry” realistically means: the goal is not perfect mirror images, but a balanced, natural look that holds up in standing, walking, and seated positions.
Surgical Techniques & Implant Placement Planes
The most important technical decision in butt implant surgery is not the brand or the “cc” number—it’s where the implant is placed (the “plane”) and how the pocket is engineered to remain stable over time. Because the buttocks are a high-motion, high-pressure area (walking, sitting, training), plane selection has a direct impact on comfort, edge visibility, implant movement, and complication risk.
Intramuscular placement (within the gluteus maximus)
Intramuscular placement positions the implant within the substance of the gluteus maximus muscle. Many surgeons favor this plane because the muscle can provide robust coverage and help stabilize the implant against visible edges—especially important for lean patients.
Potential advantages include:
- Improved coverage: Muscle can help camouflage the implant’s borders.
- Stability support: When the pocket is well designed, intramuscular placement can reduce visible shifting.
- Natural blending: Often helpful for patients with minimal subcutaneous fat.
Important trade-offs and considerations:
- More demanding technique: It requires precise dissection and symmetry control.
- Early discomfort: Patients may experience more muscle-related tightness and soreness during the first 1–2 weeks.
- Movement management: Strict activity restrictions matter—high-impact actions too early can stress the pocket.
Subfascial placement (beneath fascia, above muscle)
Subfascial placement positions the implant under the fascia (a strong connective tissue layer) but above the gluteus maximus. This plane can offer a balance between coverage and recovery comfort for selected patients.
Potential advantages include:
- Less muscle disruption: Some patients report an easier early recovery compared with deeper muscle dissection.
- Defined pocket boundaries: Fascia can provide structure to support implant position.
Important trade-offs and considerations:
- Coverage depends on your tissue thickness: In very lean patients, edges may be more noticeable.
- Higher importance of sizing discipline: Oversizing can increase edge visibility and strain the incision line.
- Pocket precision is still critical: A poorly designed pocket can increase malposition risk.
Submuscular and subcutaneous discussions (why they’re considered, and why they’re limited)
You may see terms like submuscular (beneath the muscle) or subcutaneous (beneath the skin/fat) online. In practice, these planes tend to be more limited or selectively used, because the buttock region behaves differently than other areas of the body.
- Subcutaneous placement: May increase the risk of visible edges, palpability, rippling, and higher mechanical stress on the incision—especially in thin patients.
- Submuscular placement: Can be technically challenging due to anatomy and may not provide the same practical advantages as in other implant surgeries.
For the expert patient, the key takeaway is: plane choice should be justified with a clear anatomical explanation. Ask your surgeon to describe why your tissues support that plane, how they prevent malposition, and what restrictions they recommend to protect the pocket during early healing.
| Placement Plane | Core idea | Typical strengths | Typical trade-offs |
|---|---|---|---|
| Intramuscular | Implant sits within the gluteus maximus | Strong coverage; often better edge camouflage; can improve stability in lean patients | More technically demanding; early muscle tightness/soreness; strict activity compliance needed |
| Subfascial | Implant sits under fascia, above muscle | May reduce muscle disruption; structured pocket boundary | Coverage depends on tissue thickness; sizing discipline is critical to avoid edge visibility |
| Subcutaneous (selective) | Implant sits under skin/fat | Less deep dissection | Higher risk of palpability/edge visibility; less protection under mechanical stress |

Best Procedures to Combine With Butt Implants
Butt implant surgery can be performed as a standalone procedure, but in appropriately selected patients it may also be safely paired with other body-contouring operations to create a more proportionate, “whole-body” result. The key is anatomy-first planning: combining procedures should improve harmony (waist-to-hip balance, silhouette flow, and projection) without overloading the body’s healing capacity. A thoughtful combined approach prioritizes surgical sequencing, realistic downtime, and a recovery plan you can actually follow.
Why combine butt implant surgery with liposuction?
One of the most common pairings is butt implant plus liposuction. This combination can be powerful because butt augmentation is not only about adding volume—it’s about improving contrast and transitions. Liposuction can refine areas such as the abdomen, flanks, lower back, or thighs to create a cleaner waistline and smoother contour into the buttocks, making implant projection look more natural and less “isolated.”
However, liposuction also increases total surgical stress and swelling. A safe plan limits the extent of liposuction when necessary, keeps positioning and incision protection in mind, and sets clear expectations about when you can return to sitting, work, and exercise.
Mommy makeover + butt implant: what to consider
A mommy makeover traditionally addresses post-pregnancy changes through a tailored mix of procedures—often including abdominal contouring and breast surgery. For patients who want improved gluteal projection as well, adding a butt implant may be considered in a broader plan, especially if there isn’t enough donor fat for a dramatic BBL result.
The most important consideration is recovery logistics. A mommy makeover can already involve limited mobility and activity restrictions. Adding butt implants introduces additional sitting limitations and incision-care priorities. The best candidates are those who can commit to structured help at home, have the ability to modify work duties, and understand that “more procedures” requires more disciplined recovery—not just more dramatic results.
Breast augmentation, breast implant pairing, and balance
For some patients, combining gluteal enhancement with breast shaping creates the most harmonious overall silhouette. Pairing a breast augmentation with a butt implant may appeal to patients seeking balanced upper and lower body proportions. If a breast implant procedure is planned at the same time, your surgeon should discuss how positioning during surgery, incision planning, and post-op movement restrictions will be coordinated to avoid competing recovery demands.
Because both areas can feel tight and sore early on, a combined plan should be conservative: appropriate implant sizing, clear pain-control strategy, and realistic timelines for driving, lifting, and returning to exercise.
Safety-first planning: who should stage procedures instead?
Not every patient should combine procedures. Staging may be safer when surgical time would become excessive, when medical risk factors (smoking, uncontrolled diabetes, higher anesthesia risk) exist, or when recovery restrictions would be impractical. A high-quality consultation should explain what is safe to combine in your specific case—and what should be separated to protect results and reduce complications.
Butt Implants vs BBL (Fat Transfer)
“Butt implants vs BBL” is one of the most important decision points for patients. Both procedures can create a more curvy silhouette, but they work through fundamentally different mechanisms: implants add structural volume with a device, while BBL uses your own fat to build volume and contour. The safest and most satisfying choice depends on your anatomy, your risk tolerance, and the type of result you’re aiming for.
How each procedure creates volume
Butt implants create projection with a pre-formed implant placed into a controlled pocket. The projection is typically more predictable because the volume does not rely on fat survival.
BBL (fat transfer) uses liposuction to harvest fat from donor areas (abdomen, flanks, back, thighs), processes that fat, and reinjects it to add shape and volume. The key variable is fat take (how much of the transferred fat survives long-term), which can vary by technique and patient biology.
Best candidates: when implants win, when BBL wins
Implants are often preferred when:
- You are very lean and lack adequate donor fat for meaningful augmentation.
- You want a clear increase in projection without relying on fat survival.
- You want a stable “framework” and are willing to follow strict sitting/activity restrictions early on.
BBL is often preferred when:
- You have adequate donor fat and want to improve buttock volume and overall contour (waist-to-hip shaping).
- You prefer avoiding implants and accept that fat survival may be partial.
- You want broader contouring that extends into hips and transitions (not just projection).
Results, feel, and longevity
Feel: BBL results often feel “tissue-like” because it is your own fat. Implants can still look and feel natural when sized and placed correctly, but the result is a device-based augmentation.
Predictability: Implants typically provide more predictable projection. BBL has a variable component due to fat survival, meaning the long-term size may decrease from the early post-op appearance.
Longevity: Both can be long-lasting. With implants, longevity depends on implant integrity and long-term tissue behavior (capsule formation, malposition risk). With fat transfer, long-term maintenance depends on stable weight and the amount of fat that permanently survives.
Safety profile and the “risk reality” expert patients should know
All surgery has risks. A trustworthy consultation acknowledges those risks and explains prevention strategies.
- Butt implants risk themes: infection, wound healing problems (especially near the crease incision), fluid collection (seroma), capsular contracture, and malposition/displacement.
- BBL risk themes: risks associated with liposuction plus fat transfer. Expert patients should specifically ask about the surgeon’s injection plane strategy and safety protocols, because safety depends heavily on technique.
If you are comparing options, the best question is not “Which is safer in general?” but “Which is safer for me, with my anatomy and my surgeon’s technique?” A high-quality surgeon should be able to explain the risk drivers and the exact steps they take to reduce them.
| Factor | Butt Implants | BBL (Fat Transfer) |
|---|---|---|
| Best for | Lean patients; strong projection goals; predictable structural volume | Patients with donor fat; desire for waist/hip contouring and softer transitions |
| Predictability | Typically more predictable projection | Variable due to fat survival |
| Scars | Usually hidden crease incision | Small liposuction access sites |
| Key trade-offs | Device-based; pocket stability and incision healing are critical | Depends on donor fat and technique; results may change with weight and fat take |
| Common concern keywords | Malposition, capsular contracture, infection, “gone wrong” scenarios | Fat survival variability, contour irregularities, liposuction recovery |
Many patients ultimately choose one path based on anatomy (fat availability) and risk preferences. In selected cases, a hybrid strategy may be used—an implant for projection with conservative fat grafting to soften transitions—but this requires careful planning and realistic expectations.
Anesthesia Options, Pain Control & Patient Comfort
For butt implant surgery, anesthesia planning is not a “small detail.” It directly affects safety, comfort, and how smoothly you recover in the first 24–72 hours. Most butt implant procedures are performed under general anesthesia because they require precise positioning, controlled muscle relaxation (in many cases), and a sterile surgical field that is difficult to maintain comfortably while awake. The goal is a stable, closely monitored experience—before, during, and after surgery.
General anesthesia for butt implants (why it’s commonly used)
General anesthesia means you are fully asleep and continuously monitored by an anesthesia team. For butt implants, this is commonly preferred because:
- Positioning is critical: You may be positioned prone (face down) or in a modified position that must remain stable for pocket accuracy and symmetry.
- Controlled movement improves precision: A motion-free field helps the surgeon create a symmetric pocket and reduce tissue trauma.
- Muscle-related steps may require relaxation: In intramuscular planning, the surgeon’s ability to work with consistent muscle tone can matter.
Expert-patient questions to ask include:
- Who provides anesthesia care (board-certified anesthesiologist vs anesthesia team model)?
- What monitoring is used during surgery (standard of care should include continuous vital monitoring)?
- How is nausea prevented (antiemetics, hydration plan)?
- What is the post-op pain strategy for the first 48 hours?
Alternative anesthesia frameworks (and why they are usually limited for this procedure)
Some cosmetic procedures can be performed under twilight sedation (deep sedation with local anesthesia) or “awake” frameworks in carefully selected cases. For butt implants specifically, these alternatives are less commonly appropriate due to positioning demands, procedural duration, and the need for consistent surgical control.
If you see marketing language suggesting “awake” options for many surgeries, treat it as a starting point for conversation—not an automatic fit for butt implants. The safer approach is individualized anesthesia selection based on:
- Procedure complexity and duration
- Your health profile (airway, sleep apnea, cardiopulmonary status)
- Your anxiety level and how you respond to sedation
- Surgeon and anesthesia team preference based on safety and predictability
The “green flag” is a team that explains why a specific anesthesia plan is recommended for your case and what they do to reduce risks—rather than pushing a one-size-fits-all approach.
Pain control: what’s normal, what helps, and what to avoid
Butt implant recovery is often described as tightness, deep soreness, and pressure rather than sharp pain—especially in the first week. Pain control typically works best with a multimodal plan (several methods layered together) rather than relying on a single medication.
Common components of a responsible pain plan include:
- Scheduled non-opioid medications (as appropriate) to reduce baseline inflammation and pain
- Short-course stronger pain medication for breakthrough pain during early recovery
- Careful mobility guidance (walking early, but avoiding strain and pressure)
- Positioning strategies to protect the incision and reduce pressure on the pocket
What to avoid (unless your surgeon explicitly approves): overexertion, early sitting pressure, aggressive stretching, and returning to high-impact activity too soon. Many “butt implants gone wrong” scenarios are not dramatic overnight events; they can start as small wound stress or pocket strain in the first 2–3 weeks when tissues are still fragile.
Step-by-Step: How Butt Implant Surgery Works
Understanding the procedure step-by-step helps expert patients set realistic expectations and evaluate surgical quality. While techniques vary by surgeon, safe butt implant surgery is built around the same core principles: sterile planning, precise pocket creation, implant handling that minimizes contamination, and closure designed to protect a high-motion incision area.
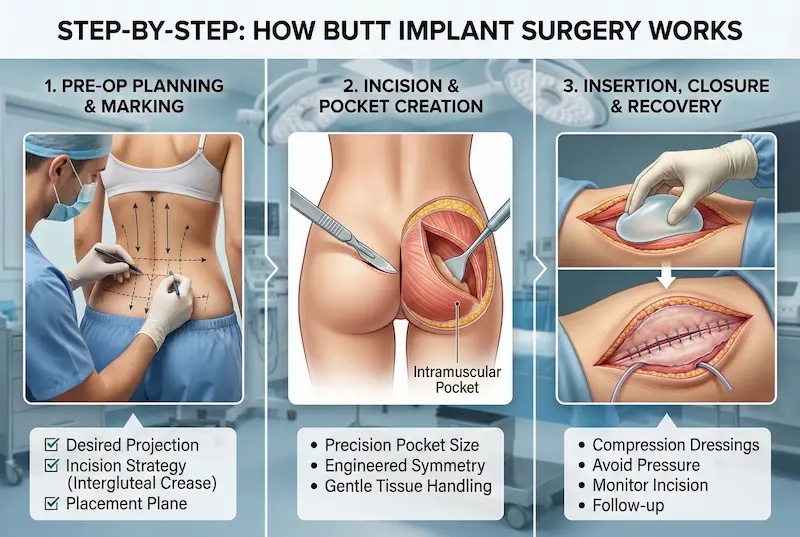
Pre-op planning, marking, and operating room setup
Before surgery, your surgeon typically confirms your goals and marks key anatomical landmarks. This includes midline reference points and symmetry guides that help align pocket design on both sides. A quality plan includes an honest review of:
- Desired projection vs tissue coverage (to reduce edge visibility and wound stress)
- Incision strategy (commonly the intergluteal crease for scar concealment)
- Placement plane (intramuscular vs subfascial) and why it fits your anatomy
On the day of surgery, you can expect a standard safety workflow: verification of procedure details, positioning checks, and sterile prep. Many clinics also use prophylactic steps such as antibiotic protocols and mechanical prevention measures for clots (based on individual risk assessment).
Incision location, pocket creation, and plane execution
The most common incision is placed within the intergluteal crease (the natural fold between the buttocks) to keep the scar hidden. From there, the surgeon creates a pocket in the predetermined plane. This is the technical heart of the procedure.
What expert patients should know about pocket creation:
- Pocket size must match implant size: Too tight can increase pressure and pain; too loose can increase shifting and asymmetry risk.
- Symmetry is engineered, not hoped for: The surgeon measures and checks both sides repeatedly during pocket work.
- Plane selection affects stability and feel: Intramuscular pockets may improve coverage, while subfascial pockets may reduce muscle disruption in selected patients.
Because this area is prone to mechanical stress (sitting and movement), pocket precision and gentle tissue handling matter not just for appearance, but for wound healing and long-term stability.
Implant insertion, closure, drains, and dressings
Once the pocket is ready, the implant is inserted using sterile handling techniques. The surgeon then confirms position and contour, checking for symmetry and edge smoothness before closing.
Closure strategy is particularly important in butt implants because the incision area experiences tension and moisture. Depending on the surgeon’s approach and your case, you may see:
- Layered closure: Multiple deep layers to reduce tension on the skin
- Drains: Sometimes used to reduce early fluid collection (seroma) risk
- Dressings and compression: Used to support healing and reduce swelling
Before you leave, you should receive clear written instructions about:
- How to sleep and move to avoid pressure on the implants
- When you can sit (and what support pillows, if any, are recommended)
- How to monitor the incision for early warning signs (increasing redness, drainage, fever)
- Follow-up schedule and how to reach your clinical team after hours
In the next section, we’ll map recovery in a practical timeline—what you can expect day-by-day and week-by-week, including the restrictions that most strongly influence safety and final shape.
Butt Implant Recovery Timeline (Day-by-Day)
“Butt implant recovery” is less about a single moment of pain and more about protecting your incision and implant pocket during a predictable healing window. The first 2–6 weeks are the highest-leverage phase: what you do (and don’t do) during this time can influence comfort, wound healing, swelling, and long-term implant stability. A safe recovery plan combines smart positioning, gradual mobility, incision hygiene, and a disciplined return-to-activity schedule.
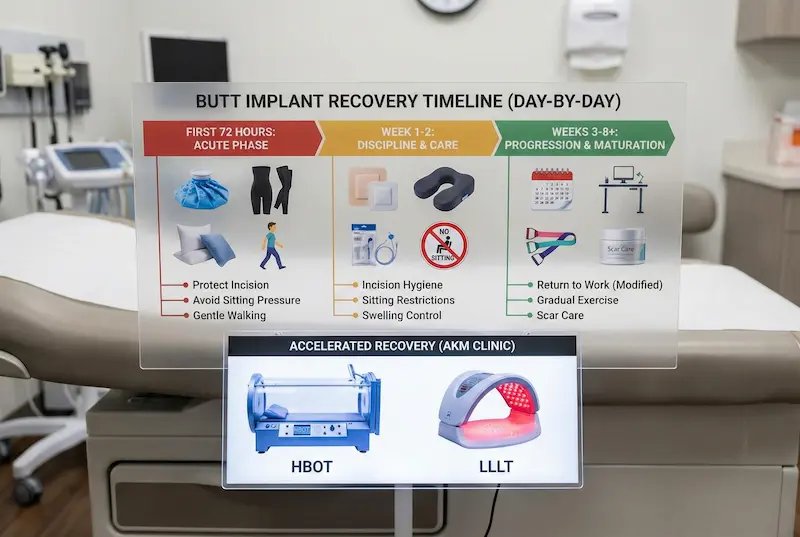
First 72 hours: swelling, tightness, mobility, and positioning
The first three days are typically the most intense. Most patients describe a deep soreness and tightness that feels “pressure-like,” especially when changing positions. Your priorities in this phase are:
- Protect the incision: Keep the area clean, dry, and avoid friction. Follow your surgeon’s dressing instructions exactly.
- Reduce pressure on the pocket: Avoid sitting directly on the implants unless your surgeon gives specific guidance. When you must sit briefly, use the support strategy recommended by your surgical team.
- Walk early, but gently: Short, frequent walks help circulation and reduce clot risk. The goal is movement without strain.
- Sleep positioning matters: Many surgeons recommend sleeping on your stomach or sides (depending on the case) to avoid direct pressure. Use pillows to stabilize your position.
- Hydration and nausea control: Hydration supports healing and helps minimize dizziness or constipation from early medications.
What is “normal” in the first 72 hours can include swelling, tightness, bruising, and fatigue. What is not normal and should be reported: rapidly increasing redness, fever, foul-smelling drainage, severe one-sided swelling, or shortness of breath.
Week 1–2: incision care, sitting rules, drains (if used), and swelling control
Week 1 is often the point where expert patients realize recovery is a discipline. The implants may feel “high,” firm, or tight as swelling and tissue stiffness peak. The key is to protect the incision line and pocket while your body stabilizes the tissues around the implant.
- Sitting restrictions: This is the biggest behavior change. Many surgeons limit direct sitting pressure early to protect the incision and reduce pocket stress. If you work at a desk, plan ahead (standing desk, modified schedule, time off).
- Hygiene and incision management: Follow your surgeon’s instructions on showering, wound care, and when dressings can be changed.
- Garments/support: If compression or supportive garments are prescribed, use them exactly as directed. Over-compression or improper fit can create uneven pressure.
- Drains (if used): Some surgeons use drains to reduce early fluid collection (seroma). If you have them, drain care and measurement become part of daily routine until removal.
- Swelling expectations: Swelling often remains significant in week 1 and gradually begins to settle during week 2. Visible “final shape” is not expected yet.
Many patients can do light daily activities in this window, but “feeling better” does not mean tissues are ready for strain. Early overconfidence is a common driver of wound stress and pocket irritation.
Weeks 3–8+: return to work, exercise timing, and what “healed” really means
By weeks 3–4, most patients notice meaningful improvement in comfort and mobility. Swelling continues to resolve, and the implants begin to feel more “integrated” as the body adapts. However, internal healing is still ongoing. Your plan typically focuses on gradual progression.
- Return to work: Many patients return to non-physical work earlier with accommodations. Jobs that require prolonged sitting or heavy lifting usually need more time or modification.
- Exercise: Light walking is usually encouraged early. Higher-impact activity, glute-focused training, and heavy lower-body lifting typically require a longer clearance window. The surgeon’s timeline matters because pocket stability and incision maturation are individual.
- Swelling and firmness: It’s common for the area to feel firm or “tight” for weeks. Gradual softening occurs over time.
- Scar maturation: Incisions usually look their “worst” before they look better. Scar care often becomes more relevant after the incision is fully closed and cleared for topical management.
Most expert patients do best when they treat recovery like a protocol: clear milestones, conservative behavior early, and predictable progression rather than rushing the timeline.
Accelerated Recovery & Safety Protocol: HBOT + LLLT (AKM Clinic)
Some patients—especially those who prioritize minimizing visible downtime—ask about “advanced recovery” options. AKM Clinic’s recovery philosophy positions technology not as a marketing add-on, but as a structured protocol aimed at faster healing and risk reduction through two complementary therapies: Hyperbaric Oxygen Therapy (HBOT) and Low-Level Laser Therapy (LLLT).
HBOT (Hyperbaric Oxygen Therapy) is described by the clinic as exposure to 100% oxygen in a pressurized environment to super-saturate plasma oxygen and support healing in tissues where circulation may be temporarily compromised. In AKM Clinic’s internal technology analysis, HBOT is associated with patient-centric benefits such as reduced inflammation and “social downtime,” enhanced scar healing through fibroblast stimulation, and a dual defense against infection (an oxygen-rich environment that is hostile to some bacteria while supporting immune response). Suitability and timing depend on your surgical plan and medical profile.
LLLT (Low-Level Laser Therapy) is presented as a targeted cellular-level intervention. AKM Clinic describes an LLLT platform that uses medical-grade laser diodes (distinguished from simple LEDs) and a validated therapeutic wavelength, with benefits framed around cellular repair support (ATP), collagen synthesis via fibroblast stimulation, and serving as an adjunct to HBOT for a smoother visible recovery pathway.
Importantly for expert patients: AKM Clinic’s own clinical case analysis frames HBOT + LLLT as an accelerated recovery pathway used when minimizing downtime is a priority, rather than a one-size-fits-all standard for every patient. Your plan should be individualized, explained, and medically justified.
| Recovery Phase | What you may feel | Your priorities | Common mistakes to avoid |
|---|---|---|---|
| Days 1–3 | Tightness, soreness, swelling, fatigue | Protect incision, avoid pressure, short walks, proper sleep positioning | Sitting too early, twisting/straining, skipping mobility |
| Week 1 | Peak swelling, stiffness, “high” feeling implants | Strict recovery compliance, wound hygiene, follow-up, drain care (if used) | Overconfidence, friction/moisture on incision, too much activity |
| Week 2 | Gradual improvement; still swollen | Continue restrictions, progressive mobility, monitor for red flags | Returning to gym, long sitting sessions, ignoring new redness/drainage |
| Weeks 3–8+ | More comfort; swelling continues to resolve | Gradual return to activity, scar maturation plan, surgeon clearance for exercise | Heavy lower-body lifting too soon, high-impact sports, rushing “final shape” expectations |
Scars, Sensation Changes & Long-Term Maintenance
Concerns about butt implant scars and long-term “feel” are some of the most common questions expert patients research before choosing a surgeon. The key is to understand what is typical, what is avoidable with good technique and disciplined recovery, and what changes over time as scars mature and tissues adapt around the implant.
Butt implant scars: where they are and what to expect
Most butt implant procedures use an incision placed within the intergluteal crease (the natural fold between the buttocks). The main advantage is concealment: when healed well, the scar typically sits in a shadowed area that is not easily visible in daily life or in most clothing.
What expert patients should realistically expect:
- Early scar appearance is not the final scar: Scars often look more noticeable before they improve. Redness and firmness can persist for weeks.
- Moisture and friction matter: Because the incision sits in a fold, local hygiene and keeping the area as dry as safely possible (per your surgeon’s instructions) can influence healing.
- Scar quality varies by biology: Genetics, skin type, and personal healing patterns strongly affect scar maturation.
Common reasons scars may become more noticeable include wound tension, early sitting/strain, infection, or delayed wound healing. Your surgeon’s closure strategy and your early recovery discipline are major controllable factors.
Scar care: what helps (and when to start)
Scar care should be timed appropriately. Many scar products are only recommended after the incision is fully closed and your surgeon confirms it is safe to begin. In general, scar optimization strategies may include:
- Silicone-based scar therapy (gel or sheets), often used once the incision is closed and stable
- Gentle cleansing and meticulous hygiene in the crease area to reduce irritation
- Avoiding smoking and nicotine, which can significantly increase wound-healing complications
- Reducing friction through appropriate clothing choices and avoiding early activities that stress the incision line
If you are prone to thickened scarring, tell your surgeon early. Expert-level planning includes discussing scar history (keloids/hypertrophic scars), and outlining what interventions may be used if your scar becomes raised or symptomatic.
Numbness, tightness, and sensation changes
Temporary sensation changes can occur after butt implant surgery. Patients may describe:
- Numbness or reduced sensation near the incision or in adjacent skin
- Tightness, especially during the first 1–3 weeks as swelling peaks and tissues adapt
- Occasional nerve “zingers” (brief sharp sensations) as nerves recover
In most cases, these changes improve gradually as swelling resolves and tissues heal. A slower recovery of sensation can occur because superficial sensory nerves are sensitive to stretching and local inflammation.
What should prompt a call to your surgeon:
- New or rapidly worsening one-sided pain after an initial improvement
- Expanding redness, warmth, or drainage near the incision
- Sudden change in implant position or a new visible contour abnormality
Long-term maintenance: how to protect results and reduce revision risk
Butt implants are designed for long-term augmentation, but your tissues continue to age and change. Long-term satisfaction is often highest when patients adopt a “maintenance mindset”:
- Keep weight stable: Major weight gain/loss can change how tissues drape over the implant and can affect contour.
- Return to training gradually: High-impact activity too soon can stress the pocket. Long-term, most patients can train normally once cleared, but the early timeline is critical.
- Monitor for subtle changes: Persistent asymmetry, new firmness, or discomfort can be early indicators of issues like capsular tightening or malposition.
Common triggers for revision consultation can include persistent asymmetry, visible implant edges, displacement, or capsular contracture symptoms. The best protection is a conservative implant plan, stable pocket design, and strict early recovery compliance.
Risks, Complications & “Butt Implants Gone Wrong”
Expert patients search “butt implants gone wrong” because they want to understand worst-case scenarios before committing. That is a rational approach. Butt implants can be safe and effective in appropriately selected patients, but they are still major surgery in a high-motion, high-pressure area—meaning risk prevention is heavily dependent on surgical technique, sterile discipline, and recovery compliance.
Early complications (first days to first few weeks)
Early complications typically relate to wound healing, infection control, and fluid management. Potential early risks include:
- Infection: Can present with fever, increasing redness, warmth, pain, or drainage. Severe infections may require surgical intervention.
- Seroma (fluid collection): Swelling or fluid accumulation that may require drainage or monitoring.
- Hematoma (bleeding/collection): Less common, but can cause swelling and pain and may require urgent evaluation.
- Wound-healing problems: The intergluteal crease incision is exposed to tension, moisture, and movement. Wound separation (dehiscence) can occur if stressed early or if healing is impaired.
- Skin irritation or breakdown: Often related to friction, moisture, or inadequate aftercare protocols.
Prevention is not luck. It usually involves careful patient screening, meticulous sterile technique, appropriate antibiotic protocols, gentle tissue handling, pocket accuracy, and strict post-op instructions around sitting and activity.
Late complications (weeks to months and beyond)
Later complications are often related to how the body forms and remodels scar tissue around the implant, and how stable the pocket remains over time. Potential late risks include:
- Capsular contracture: Tightening or thickening of scar tissue around the implant, which may cause firmness, discomfort, or shape distortion.
- Implant malposition or displacement: Shifting that can create asymmetry, visible edges, or a “double contour.”
- Palpability or edge visibility: More likely in very lean patients or when the implant is oversized relative to tissue coverage.
- Chronic discomfort: Sometimes related to pocket tension, scar behavior, or muscle adaptation in certain planes.
For the expert patient, these risks reinforce why plane selection and sizing discipline are not cosmetic preferences—they are structural safety decisions.
What “gone wrong” often looks like (and what causes it)
When butt implants go wrong, it is often due to one or more identifiable drivers rather than an unpredictable mystery. Common “gone wrong” patterns can include:
- Visible asymmetry or shifting: Often linked to pocket design, early pressure/strain, oversizing, or inadequate stabilization.
- Wound breakdown in the crease: Often driven by early sitting pressure, friction/moisture, smoking/nicotine, infection, or excessive tension on closure.
- Overdone appearance or visible implant edges: Commonly related to oversizing, insufficient tissue coverage, or suboptimal plane choice.
- Persistent hardness/distortion: Can be a capsular contracture pattern that may progress over time.
One of the most important prevention strategies is choosing a surgeon who can clearly explain how they reduce these specific failure modes—especially pocket control, infection prevention, incision protection, and recovery rules designed for real life (work, sitting, travel).
Red flags: when to contact your surgeon (or seek urgent care)
Call your surgeon promptly if you experience:
- Fever, chills, or flu-like symptoms
- Increasing redness, warmth, or foul-smelling drainage from the incision
- Sudden, severe pain or rapidly increasing swelling on one side
- A sudden change in buttock shape suggesting implant shift
Seek urgent medical evaluation if you have:
- Shortness of breath, chest pain, or fainting
- Severe calf pain/swelling (possible clot risk)
Safety systems that reduce risk (what to look for in a provider)
Risk reduction is multi-layered: patient selection, sterile environment, intraoperative monitoring, and disciplined follow-up. When evaluating a provider, look for evidence of:
- Strict pre-operative screening: Clinics that screen candidacy carefully reduce avoidable wound and anesthesia risks.
- International sterilization standards: A documented approach to hygiene and infection prevention is foundational.
- Continuous vitals monitoring: Advanced monitoring throughout procedures is a safety baseline, not a luxury.
- Clear revision strategy: Your surgeon should be able to explain what they do if malposition, seroma, or infection occurs.
- Accessible aftercare: Rapid response to early warning signs can prevent small problems from becoming major complications.
As an example of how some clinics frame this, AKM Clinic describes its surgical environment as built around ISO/TÜV sterilization standards, advanced patient vitals monitoring, and strict pre-operative health screenings—all aimed at reducing preventable complications and improving predictability, particularly for international patients who value structured protocols and continuity of care.
Real Results (Before/After): What “Natural-Looking” Butt Implants Actually Mean
Most patients don’t want a “bigger butt” at any cost—they want a result that looks believable on their frame, moves naturally, and doesn’t broadcast “implant.” In AKM Clinic’s internal analysis of patient expectations, a consistent theme across international patients is the fear of an unnatural, “operated” look and the priority placed on naturalism. While those case studies focus on facial surgery, the core aesthetic psychology applies equally to body contouring: enhancement should look authentic, not artificial.
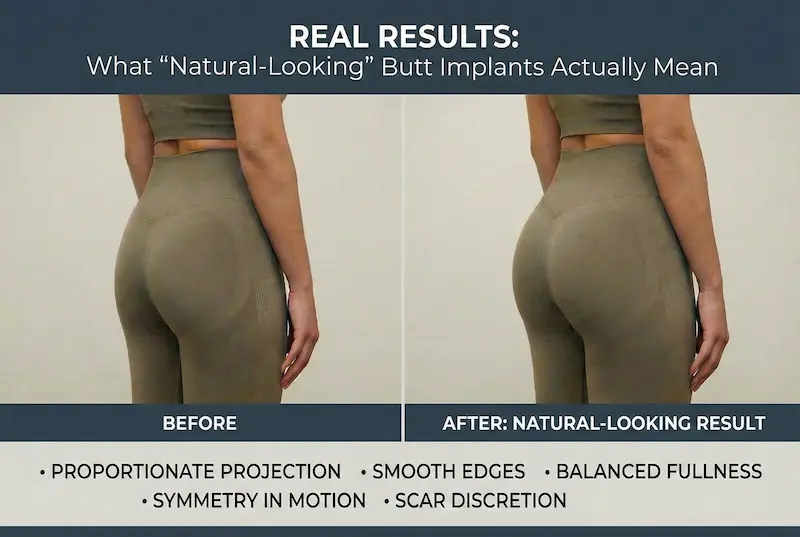
What “natural-looking” butt implants mean in practical terms
A natural-looking butt implant result is less about a trendy silhouette and more about proportion, edge control, and stable pocket design. In real life, “natural” typically means:
- Proportionate projection: The buttock matches waist, hips, and thigh transition (not an isolated “bubble”).
- Smooth edges: No visible implant outline when standing, walking, or wearing fitted clothing.
- Balanced upper-to-lower pole fullness: Fullness is distributed in a way your anatomy can support.
- Symmetry that holds up in motion: Small asymmetry is normal, but the result should not look uneven when you move.
- Scar discretion: The incision is placed and closed to heal quietly (usually within the intergluteal crease).
Surgeon’s Insight: The goal is rejuvenation, not alteration—enhancing your own proportions rather than forcing an artificial shape.
How to evaluate before/after photos like an expert patient
Marketing galleries often show a single angle, perfect lighting, and posed posture. For butt implants, you want “proof of reality.” If a clinic offers a gallery, look for variety and consistency:
- Multiple angles: front (hip/outer thigh transition), side (projection), and 3/4 angles.
- Neutral posture: Standing naturally (not exaggerated arching).
- Different clothing contexts: Results should look smooth in fitted clothing, not only in underwear.
- Timepoints: Early swelling can mislead. Prefer galleries that show longer-term healing, not only “two-week wow” photos.
- Consistency across many patients: One great result matters less than repeated, stable-looking outcomes.
In consultation, ask to see results in patients with a similar body type to you (tissue thickness, BMI range, athletic build vs softer coverage). That is far more predictive than copying a celebrity reference photo.
Common “unnatural” outcomes and what usually causes them
When butt implants look unnatural, it’s usually due to identifiable planning errors—not mystery. Common drivers include:
- Oversizing: More volume than your tissues can cover leads to visible edges and a “bolted-on” look.
- Suboptimal plane choice for your coverage: Thin patients are at higher risk of edge visibility if coverage is insufficient.
- Pocket instability: A pocket that’s too loose can contribute to shifting and asymmetry.
- Ignoring the lateral transition: Projection without addressing contour transitions (hips/outer thigh) can look abrupt.
The “best” result is usually the one created by the most disciplined plan: conservative sizing, stable pocket engineering, and a recovery protocol you can realistically follow.
Cost Analysis: Butt Implants Cost in the USA vs Turkey 2026 (Value, Not Price)
Cost research is part of being an expert patient. But cost only becomes meaningful when you understand what it includes: surgeon experience, anesthesia model, facility standards, implant quality, follow-up structure, and what happens if you need additional care. The goal is not to find the lowest number—it’s to understand value and risk management.
What actually drives the total cost
Butt implant quotes vary widely because “butt implants” can mean different surgical plans and different safety environments. Key cost drivers include:
- Surgeon expertise and specialization: Gluteal implants are technically demanding; experience is a meaningful variable.
- Facility and anesthesia fees: These can add thousands beyond surgeon fee.
- Implant costs: Brand/type and supply chain traceability matter.
- Complexity: Primary implants vs revision, and whether additional contouring (e.g., liposuction) is added.
- Aftercare structure: Follow-up visits, medications, garments, and complication-response availability.
USA cost snapshots (national average vs major metros)
For grounding, here are two commonly cited U.S. reference points:
- ASPS average surgeon fee: $7,964 for buttock implants (surgeon fee only; excludes anesthesia/facility/other costs).
- RealSelf patient-reported average: $13,454 average, with a wide reported range ($7,035–$25,001).
| Reference Point | What it represents | Typical number (USD) | Notes for expert patients |
|---|---|---|---|
| ASPS (butt implants) | Average surgeon fee | $7,964 | Does not include anesthesia, OR facility fees, or other related costs. |
| RealSelf (national) | Patient-reported total cost average | $13,454 | Based on member reviews; ranges are wide and reflect market variability. |
| RealSelf (New York City) | Patient-reported metro average | $11,375 | Metro averages can differ from state averages and vary by provider tier. |
| RealSelf (Miami) | Patient-reported metro average | $11,071 | High-volume markets can show pricing spread; focus on credentials and safety. |
| RealSelf (Los Angeles) | Patient-reported metro average | $13,737 | Premium markets may price higher due to overhead and demand. |
Important: A “cheap” quote can become expensive if aftercare is weak or if revision becomes necessary. Always ask for an itemized, all-in quote and what happens if complications occur.
Turkey value equation: why prices can be lower (and what to verify)
When patients compare “butt implants turkey” to U.S. hubs like NYC, Miami, or Los Angeles, the most important question is: why is it cheaper? AKM Clinic’s internal value framework answers this directly: the price difference is largely driven by macroeconomic factors—most notably the USD-to-TRY exchange rate and lower national operational costs—not by an intentional downgrade in standards. The clinic further positions quality assurance through the use of FDA-approved materials and operating in JCI-accredited hospitals.
Separately, some medical tourism platforms list typical advertised package ranges for butt implants in Turkey in the low-to-mid thousands (USD). Treat these as starting points, not guarantees: inclusions, implant brand, and revision coverage vary widely by provider.
| When comparing “USA vs Turkey” | What to ask (non-negotiables) |
|---|---|
| What is included? | Surgeon fee, anesthesia, facility/OR, implants, tests, garments, meds, follow-up plan. |
| Where is surgery performed? | Accredited hospital/surgical center, sterility standards, emergency capability. |
| What is the implant plan? | Plane choice rationale (intramuscular/subfascial), pocket stabilization strategy, sizing discipline. |
| Aftercare continuity | How follow-up is handled after you fly home, response speed if you have concerns. |
Choosing the Right Surgeon & Facility for Butt Implants
If you’re searching “best butt implant surgeons” or comparing providers in NYC, Miami, or Los Angeles, you’re already thinking like an expert patient: credentials, facility standards, and complication-management plans matter as much as aesthetics. Butt implants are technically demanding because the pocket must remain stable in a high-motion, high-pressure area. That’s why surgeon selection should be based on verifiable markers of expertise and a structured safety environment—not marketing photos alone.
Credentials checklist: what to verify (not just “years of experience”)
When evaluating a surgeon for butt implants, look for indicators that predict consistent outcomes and safer decision-making:
- Board certification (or equivalent): Ask what certification framework applies and how it is verified.
- Procedure-specific experience: Butt implants are different from general “body contouring.” Ask how often the surgeon performs gluteal implants and what their revision rate looks like.
- Revision capability: A strong surgeon can explain how they handle malposition, wound issues, seroma, and capsular concerns.
- Ethical sizing discipline: The best surgeons say “no” to oversizing when tissue coverage cannot support it safely.
- Clear anatomy-based plan: The surgeon should explain the placement plane and pocket strategy in plain language.
Expert tip: “Confidence” is not a credential. You want a surgeon who can explain the risks you’re worried about—openly—and show you how their technique and protocols reduce those exact failure modes.
Facility standards: what a safe environment should include
The facility matters because butt implant outcomes are influenced by sterile discipline, monitoring, and aftercare systems. At a minimum, you want a setting with:
- Accredited surgical environment: Ask where the surgery is performed and what accreditation applies.
- Intraoperative monitoring: Continuous monitoring is a baseline expectation for patient safety.
- Infection prevention systems: Sterilization standards and documented protocols reduce preventable complications.
- Pre-op screening: Candidacy screening reduces wound-healing risk, anesthesia risk, and avoidable “bad fit” cases.
- Structured post-op access: Clear follow-up schedule and rapid-response communication if you develop symptoms.
For patients comparing domestic vs international care, the facility question becomes even more important: “Where would I be treated if I needed urgent evaluation?” A trustworthy provider answers that clearly.
Questions to ask in consultation (high-signal questions)
Bring these questions to your consult. They quickly reveal whether the plan is anatomy-driven and safety-led:
- Which placement plane are you recommending for me, and why? (Intramuscular vs subfascial should be justified by tissue coverage and lifestyle.)
- How do you design the pocket to reduce malposition? (You want a clear method, not vague reassurance.)
- Where is the incision placed, and how do you protect it during healing? (Butt implant incision care is a major risk lever.)
- What is your protocol for seroma, infection, or wound separation? (Ask what happens “if X occurs.”)
- What restrictions do you require for sitting and activity, and for how long? (If restrictions are unrealistic, outcomes suffer.)
- How do you manage aftercare if I’m traveling? (Continuity of care should be defined, not implied.)

The Medical Journey in Istanbul (Logistics for International Patients)
For international patients, the medical journey is part of the procedure’s overall safety and comfort. A well-designed process reduces stress, improves compliance, and makes recovery more predictable—especially in the first week when you need structure and rapid access to guidance. The best model combines clear planning, reliable transportation, coordinated testing, and long-term follow-up after you return home.
Virtual consult → personalized plan with transparent pricing
A strong international pathway starts with an organized remote evaluation. In a typical workflow, you’ll share photos and your goals, discuss candidacy, and receive a plan that clarifies:
- Whether implants, BBL, or a hybrid approach fits your anatomy and goals
- Implant strategy (shape/size concept, placement plane rationale)
- Recovery constraints (time off work, sitting strategy, exercise timeline)
- Itemized inclusions so “package” pricing isn’t vague
Expert patients should insist on clarity: what’s included, what’s not included, and what the follow-up structure looks like once you’re back in the U.S.
Arrival, transfers, hotel, and procedure-day flow
In an all-inclusive international model, logistics are designed to eliminate friction: airport pickup, hotel coordination, and clinic transfers are scheduled so you can focus on preparation and recovery. A typical timeline includes:
- VIP airport welcome and private transfer to your hotel
- In-person consultation to confirm the surgical plan
- Pre-operative tests prior to surgery
- Procedure day in an accredited facility with structured monitoring
- Post-op recovery support with clear instructions and access to help
For butt implants specifically, your early days should be engineered for recovery compliance: minimizing unnecessary movement, having the right sleep setup, and reducing pressure on the incision and pocket.
Long-term follow-up back home: continuity of care matters
One of the biggest fears in medical travel is “post-op abandonment.” A strong program defines follow-up before you ever board a plane. In AKM Clinic’s described model, a dedicated patient host remains available via WhatsApp during recovery in Istanbul and schedules virtual surgeon follow-ups after you return home at 1, 3, 6, and 12 months.
This matters for butt implants because some concerns don’t appear on day 3—they can develop over weeks (persistent swelling, scar issues, asymmetry signals, or capsular tightening symptoms). A structured follow-up plan helps catch problems early, when intervention is simpler.
FAQ: Butt Implants
These are the most common “real-world” questions patients ask when researching butt implants. The answers below are designed to be direct, practical, and medically grounded—so you can make decisions with clarity, not marketing.
Are butt implants safe?
Butt implants can be safe for appropriately selected patients when performed by an experienced surgeon in an accredited, well-monitored surgical environment. Safety depends heavily on candidate selection (health status, tissue coverage, nicotine use), sterile technique, pocket accuracy, and recovery compliance (especially avoiding early sitting pressure and strain).
Ask your surgeon to explain the specific risks they focus on preventing—like infection, wound healing problems in the crease incision, fluid collection (seroma), and implant malposition—and what their protocol is if any of these occur.
What are butt implants made of?
Most butt implants are made of medical-grade silicone engineered to be durable and shape-stable in a high-motion, high-pressure area. The device is designed specifically for gluteal augmentation, with material properties intended to withstand sitting and muscle movement over time.
As an expert patient, you should request documentation of the implant type and traceability, and understand why your surgeon chose that specific implant concept for your anatomy.
How long do butt implants last?
High-quality butt implants are designed to be long-lasting and many patients keep them for years. However, no implant is guaranteed to last forever. Long-term outcomes depend on factors like tissue behavior, capsule formation, pocket stability, and lifestyle.
Some patients pursue revision in the future due to capsular contracture, malposition/asymmetry, changes in aesthetic preferences, or body changes over time.
What is butt implant recovery like week by week?
Recovery is usually most intense in the first week, with tightness, swelling, and deep soreness. Weeks 1–2 often require the strictest compliance: protecting the incision in the crease, minimizing pressure, and following sitting/activity restrictions. By weeks 3–4, many patients feel significantly better, but internal healing continues for weeks.
Your surgeon’s timeline matters. Returning to heavy lower-body training or prolonged sitting too soon can stress the pocket and incision before tissues are ready.
Butt implants vs BBL: which looks more natural?
Either can look natural when planned correctly. A BBL can feel and behave like natural tissue because it uses your own fat and can contour surrounding areas (waist/hips). Butt implants can also look natural when sizing is conservative, tissue coverage is adequate, and the pocket is stable—so edges are not visible and projection matches your proportions.
The more useful question is: which option matches your anatomy and goals? Lean patients with limited donor fat often get more predictable projection from implants, while patients with adequate donor fat may prefer fat transfer for broader shaping.
Where are butt implant scars located?
Most surgeons place the main incision within the intergluteal crease (the natural fold between the buttocks) to keep the scar hidden. Scar quality depends on closure technique, your biology, and—very importantly—how well you protect the incision from early tension, moisture, and friction.
Scars typically improve over time. It’s normal for scars to look more noticeable before they fade and soften.
Can butt implants look and feel natural?
Yes—when the implant plan is anatomy-driven. Natural outcomes typically come from disciplined choices: an implant that fits your gluteal footprint, a placement plane that provides adequate coverage, and a pocket designed to hold the implant securely without shifting.
Unnatural outcomes are commonly linked to oversizing, insufficient tissue coverage, or a pocket that is too loose (increasing movement and asymmetry risk).
What are the most common butt implant complications?
Complications can include infection, seroma (fluid collection), wound healing problems at the crease incision, capsular contracture, implant malposition/displacement, and visible edges in patients with limited coverage. Many of these risks are reduced through careful candidate selection, sterile discipline, precise pocket engineering, and strict early recovery rules.
Ask your surgeon what warning signs they want you to report immediately (fever, increasing redness, foul drainage, sudden swelling, or a sudden shape change suggesting implant shift).
How much do butt implants cost in the USA vs Turkey?
Costs vary widely based on surgeon expertise, anesthesia/facility fees, implant selection, complexity (primary vs revision), and the structure of aftercare. In the USA, major metro markets can carry higher facility and overhead costs. In Turkey, pricing can be lower due to macroeconomic and operational cost differences, but the expert patient should still verify standards and inclusions.
The best approach is to request an itemized quote (surgeon, anesthesia, facility, implants, tests, garments, medications, follow-up plan) and confirm where the surgery is performed (accredited setting, monitoring standards, and emergency capability).
How do I choose the best butt implant surgeon?
Choose a surgeon who can clearly explain your implant plan and risk management—not just show photos. High-signal indicators include verifiable credentials, procedure-specific experience with gluteal implants, a disciplined approach to sizing, and a defined protocol for managing complications and long-term follow-up.
In consultation, ask: which placement plane they recommend for you and why, how they prevent malposition, how they protect the crease incision during healing, and what your sitting/activity timeline realistically looks like.
Do HBOT and LLLT help butt implant recovery?
Some clinics offer advanced recovery support options aimed at reducing inflammation and supporting tissue healing. At AKM Clinic, HBOT and LLLT are described as a structured “Accelerated Recovery & Safety Protocol,” positioned to support visible downtime reduction and tissue repair pathways in selected patients.
Ask whether these therapies are medically appropriate for your case, how they fit into your recovery timeline, and what outcomes the clinic expects them to support (comfort, swelling management, scar maturation support, and overall recovery experience).








