An awake breast lift is a modern approach to mastopexy (breast lift surgery) performed without full general anesthesia, typically using a carefully planned combination of local anesthesia and twilight sedation. For the “expert patient,” the appeal is simple: you’re prioritizing control, safety, and a smoother recovery experience—without compromising the core surgical goal of reshaping and lifting the breast.
This guide is designed to be a definitive medical reference. It explains the anatomy of breast ptosis (sagging), the incision patterns (donut, lollipop, anchor, crescent), what “awake” really feels like, and how to think through candidacy, risks, scars, and recovery. Along the way, you’ll also learn how high-standard clinics structure safety protocols to reduce avoidable complications and optimize healing.
Table of Contents
What Is an Awake Breast Lift?
A breast lift (mastopexy) is not a ‘one-size-fits-all’ procedure—see a clinical overview of mastopexy—it’s a surgical plan built around your anatomy, your degree of sagging, and your goals for shape, nipple position, and upper-pole fullness. The word “awake” can be misleading: it does not mean you will be fully alert, uncomfortable, or “watching surgery.” In most cases, it refers to a technique that avoids full general anesthesia and instead uses local numbing plus monitored sedation to keep you relaxed.
Breast Lift (Mastopexy) — The Medical Definition
A breast lift reshapes the breast by addressing three core issues:
- Skin envelope laxity: stretched skin that no longer supports the breast in a youthful position.
- Breast mound position/shape: tissue that has shifted downward and outward over time.
- Nipple–areola position: a nipple that sits lower on the breast and may point downward.
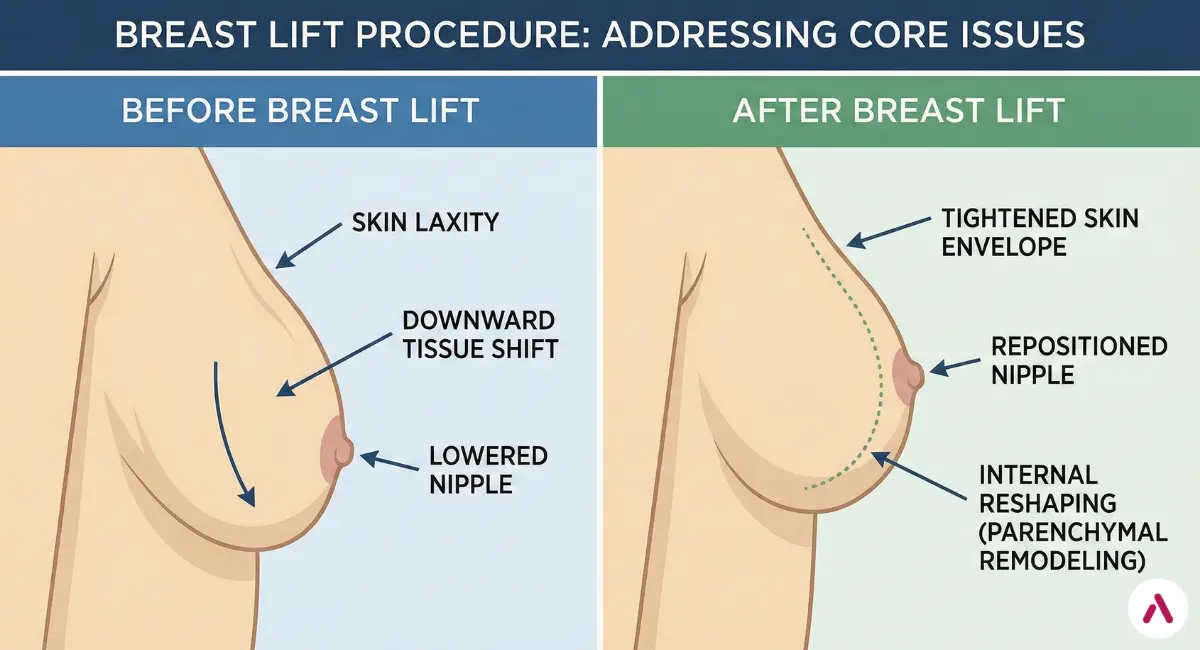
The surgery removes excess skin, tightens and re-drapes the skin envelope, and repositions the nipple–areola complex to a more youthful location while preserving blood supply. In many techniques, internal reshaping (parenchymal remodeling) is also used to create a better projection and a more stable contour.
What “Awake” Actually Means (Local Anesthesia + Twilight Sedation)
In an awake breast lift, comfort is created in layers:
- Local anesthesia: numbs the surgical field so pain signals are blocked at the tissue level.
- Twilight sedation: helps reduce anxiety and awareness. Many patients feel drowsy, calm, and have limited memory of the procedure.
- Continuous monitoring: vital signs are tracked throughout, and sedation can be adjusted based on how you’re doing moment to moment.
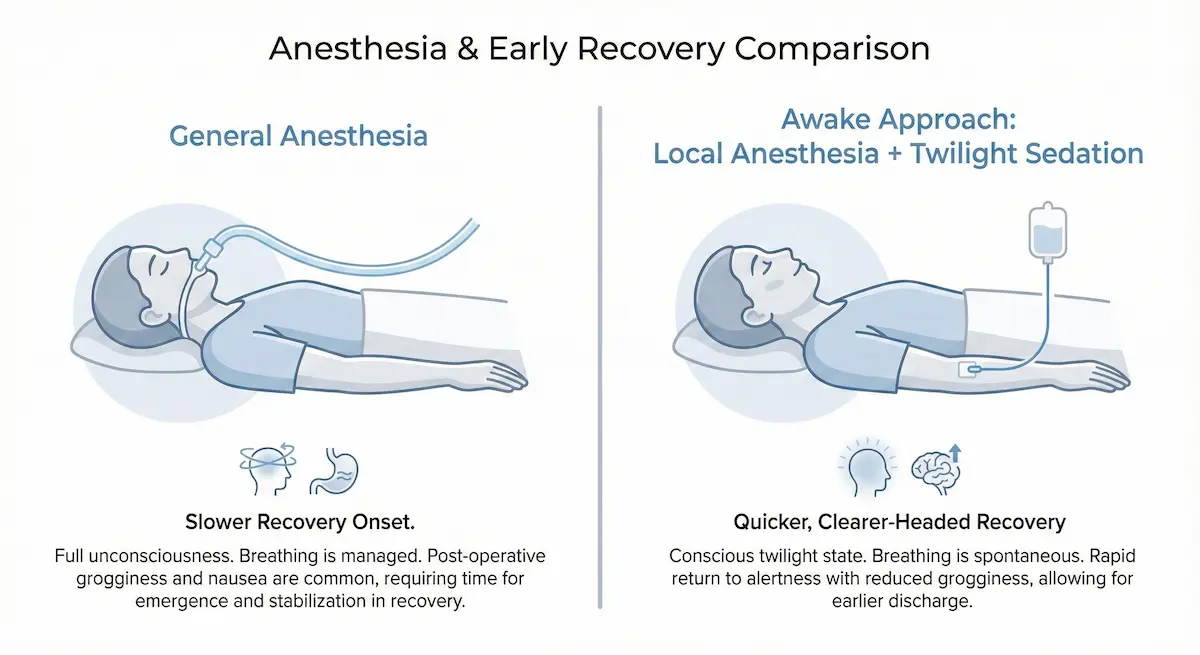
This approach is often sought by patients who want to avoid some of the common downsides of general anesthesia—such as deeper postoperative grogginess, nausea, or a longer “reset” period—while still having a controlled, medically supervised surgical experience.
Goals vs. Limits (Lift ≠ Volume Increase)
A breast lift is primarily about position and shape, not size. It can:
- Raise the breast mound and improve projection.
- Reposition the nipple–areola complex higher on the breast.
- Improve symmetry and reshape the lower pole.
- Reduce areola diameter (in selected cases).
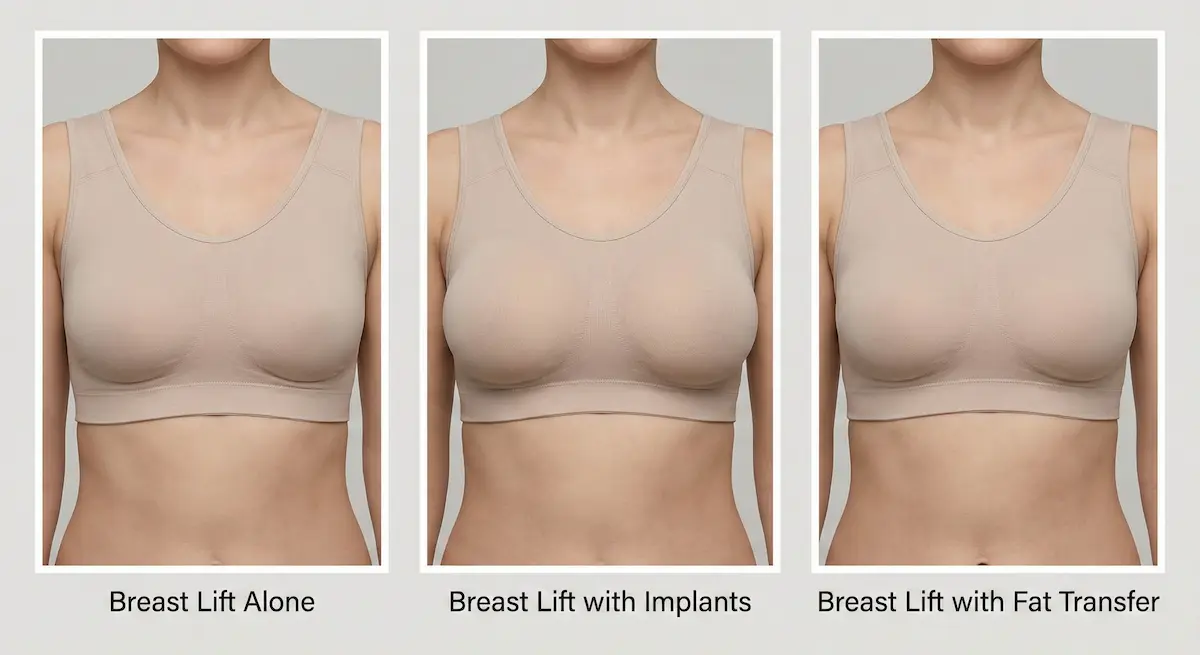
But it does not reliably create a large increase in upper-pole fullness. If your goal is a fuller upper pole, you may need a combined approach such as breast lift with implants or breast lift with fat transfer (covered later in this guide).
Breast Anatomy and the Mechanics of Ptosis
Understanding why breasts sag is the key to understanding why incision choice, internal reshaping, and scar placement differ from patient to patient. A skilled plan treats the cause of ptosis—skin stretch, tissue descent, and support weakening—not just the visible symptom.
Skin Envelope, Gland, and Support Structures (Cooper’s Ligaments)
The breast sits within a soft tissue “envelope” made of skin and internal fibrous support (commonly described as Cooper’s ligaments). Over time, this system can weaken due to:
- Pregnancy and breastfeeding changes
- Weight loss and gain cycles
- Genetics and skin elasticity
- Natural aging and gravity
When the envelope stretches beyond its ability to recoil, the breast mound “settles” lower on the chest. A mastopexy corrects this by reducing excess skin and reshaping internal tissue to better match the new, lifted position.
Nipple–Areola Complex Position and Blood Supply Basics
One of the most important safety principles in breast lift surgery is protecting the blood supply and nerve supply to the nipple–areola complex. This is why surgeons often use a “pedicle” concept (a planned tissue stalk) to maintain vascularity while moving the nipple to a higher position. Your anatomy, degree of lift, and the chosen incision pattern all influence how that pedicle is designed.
Ptosis Grades and Why They Change the Surgical Plan
Clinically, ptosis is commonly assessed by where the nipple sits relative to the inframammary fold (the crease under the breast). While grading systems vary, the key idea is consistent: more ptosis usually requires more surgical control over skin removal and reshaping, which typically means a more extensive incision pattern. This is why a minimal-scar approach is not always appropriate—even if it sounds appealing in theory.
Ideal Candidates and Who Should Wait
An awake breast lift can be a strong fit for the right patient, but “awake” is not automatically better for everyone. Candidacy depends on your anatomy, your medical history, your comfort with sedation, and the technical complexity of the lift you need.
Best Candidates (Post-pregnancy, Weight Changes, Aging)
You may be an excellent candidate if you:
- Have mild to significant sagging and want a higher, more youthful breast position.
- Notice downward-pointing nipples or areola stretching you want corrected.
- Are finished (or close to finished) with major pregnancy/weight changes.
- Prefer to avoid full general anesthesia when medically appropriate.
Factors That Increase Risk (Smoking, Unstable Weight, Uncontrolled Conditions)
Any breast lift—awake or not—carries higher risk when healing capacity is impaired. Common risk amplifiers include:
- Nicotine use (including vaping), which reduces blood flow and increases wound-healing complications.
- Uncontrolled diabetes or other conditions that impair tissue repair.
- Significant weight fluctuations, which can stretch the skin envelope again.
- Prior breast surgeries, which may change anatomy and blood supply patterns.
A safety-forward clinic will use strict pre-operative screening and clear candidacy criteria to reduce preventable complications.
When to Delay Surgery (Future Pregnancy, Goal Weight, Lactation Planning)
It may be wise to wait if you expect major hormonal or weight changes soon. Pregnancy and breastfeeding can alter breast volume and skin elasticity, potentially undoing part of the lift. Similarly, if you are actively losing weight, reaching a stable baseline first often improves both planning accuracy and long-term durability.
Breast Lift Techniques and Incision Patterns
The best breast lift technique is the one that matches your anatomy—not the one with the smallest scar on paper. Incision patterns are chosen based on the degree of sagging (ptosis), skin quality, breast volume distribution, areola size, and how much reshaping is required to create a stable, lifted contour. In general, the more lift and control you need, the more surgical “access” your surgeon needs, which usually means a more extensive incision pattern.
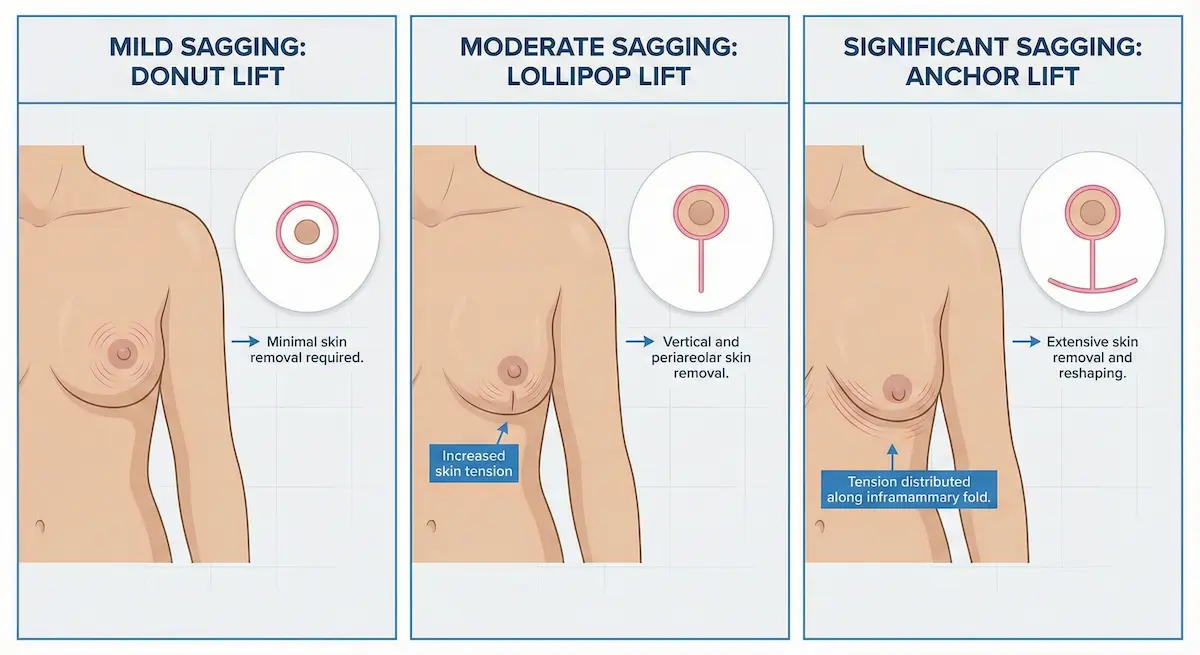
Donut (Periareolar) Breast Lift: When It Works—and Its Trade-Offs
A donut breast lift (also called a periareolar lift) uses an incision around the areola. It can be appropriate for mild sagging and for patients who want modest nipple elevation and areola resizing with a limited external scar pattern.
- Best for: Mild ptosis, mild areola enlargement, minimal reshaping needs.
- Primary advantage: Scar is confined to the areola border.
- Common limitations: Limited lifting power; can flatten the breast shape if asked to do “too much.”
- Key risk to discuss: Areolar widening or “stretching” over time if the skin is thin or tension is high.
Expert planning is especially important here: attempting a donut lift for moderate-to-severe ptosis can lead to a short-lived lift, widened areola scars, or a less ideal breast contour.
Lollipop (Vertical) Breast Lift: The Workhorse for Many Patients
The lollipop breast lift (vertical lift) combines an incision around the areola with a vertical incision down to the breast crease. It provides significantly more shaping control than a donut lift while avoiding the longer horizontal scar of an anchor pattern.
- Best for: Mild-to-moderate ptosis, moderate reshaping needs, patients seeking a balanced scar-to-lift trade-off.
- Primary advantage: Stronger lift and better shaping than donut, with a scar pattern that many patients find acceptable.
- What it’s great at: Improving projection, narrowing a widened breast footprint, and elevating the nipple–areola complex.
A vertical lift often allows more meaningful internal remodeling. For patients who want a natural-looking, lifted breast without the fullest upper pole of an implant, this technique can be an ideal middle ground.
Anchor (Inverted-T) Breast Lift: When It’s Medically Necessary
The anchor breast lift (inverted-T or Wise-pattern lift) adds a horizontal incision along the inframammary fold (breast crease) in addition to the areolar and vertical components. While many patients prefer to avoid this longer scar, the anchor approach is sometimes the most medically appropriate option because it provides the greatest control over skin removal and reshaping.
- Best for: Significant ptosis, major skin excess, substantial reshaping requirements, larger or heavier breasts.
- Primary advantage: Maximum ability to remove redundant skin and stabilize a lifted shape.
- Why surgeons choose it: Better control for severe sagging can reduce “early drop” or bottoming-out in appropriate candidates.
In practice, the anchor pattern is often chosen when a more limited incision would create too much tension, increasing the risk of widened scars, delayed healing, or an unnatural shape. The goal is not “more scars”—it’s more control with less tension.
Crescent Breast Lift: Why It’s Limited
A crescent breast lift removes a small crescent-shaped piece of skin above the areola. It can provide a very modest nipple elevation, but its use is limited because it does not allow meaningful reshaping of the breast mound.
- Best for: Very mild nipple position concerns, highly selected cases.
- Primary advantage: Minimal incision.
- Main limitation: Minimal lifting power and limited ability to correct true ptosis.
Because it can subtly change areolar shape or tension distribution, a crescent lift is typically reserved for patients who truly need only a small adjustment.
Technique Choice: A Practical Comparison Table
| Incision Pattern | Lift Power | Shaping Control | Scar Footprint | Typical Best Fit |
|---|---|---|---|---|
| Donut (Periareolar) | Low | Low–Moderate | Around areola | Mild ptosis, areola resizing |
| Lollipop (Vertical) | Moderate–High | High | Around areola + vertical line | Mild–moderate ptosis, contour improvement |
| Anchor (Inverted-T) | High | Very High | Around areola + vertical + crease line | Moderate–severe ptosis, major skin excess |
| Crescent | Very Low | Low | Small arc above areola | Very mild nipple elevation |
What Patients Often Miss: “Short Scar” vs. “Low Tension”
Many complications patients fear—wide scars, delayed wound healing, distorted areola shape—are not caused simply by the existence of a scar. They’re often related to tension and tissue quality. A well-designed plan aims to:
- Use an incision pattern that matches the amount of lift needed.
- Redistribute tension through internal shaping rather than pulling only on skin.
- Protect blood supply to the nipple–areola complex with careful pedicle planning.
That is why an experienced surgeon may recommend a more extensive incision pattern for safety and predictability—even when a minimal-scar option sounds appealing.
Awake Anesthesia Options: Local Anesthesia vs. General Anesthesia
If your primary concern is safety and recovery experience, anesthesia is not a side detail—it’s a core part of the plan. An “awake” approach is typically built around local anesthesia for pain control plus twilight sedation for comfort, with continuous monitoring throughout. The best choice depends on your medical profile, the complexity of your lift, and your personal tolerance for sedation and surgical environments.
Local (Tumescent) Anesthesia + Twilight Sedation: What It Can Feel Like
Most patients describe twilight sedation as a relaxed, drowsy state where time feels compressed. You may:
- Feel calm and sleepy, with reduced awareness of the procedure.
- Have limited memory of portions of the surgery.
- Be able to respond to simple prompts if needed (without distress).
Local anesthesia is what blocks pain. Sedation is what reduces anxiety and awareness. Together, they can create a controlled experience that avoids the “deep reset” some patients feel after general anesthesia.
General vs. Awake Approach: How the Recovery Experience Often Differs
While individual experiences vary, the practical reasons patients explore an awake breast lift often include:
- Less postoperative grogginess in the immediate hours after surgery.
- Potentially lower nausea burden compared with some general anesthesia recoveries.
- Quicker early mobilization, which can support comfort and routine activity (within medical limits).
Importantly, “awake” is not a guarantee of zero discomfort—your recovery still depends on the extent of reshaping, swelling response, and how your body heals. But for many expert patients, the anesthesia plan is a meaningful lever for improving the overall experience.
Who Is Not a Good Candidate for an Awake Breast Lift?
An awake approach can be a strong option, but it is not ideal for every patient. Reasons it may not fit include:
- High anxiety that cannot be managed safely with sedation planning.
- Complex surgical scope requiring prolonged operative time or extensive dissection.
- Medical factors where the anesthesia team determines general anesthesia provides a safer controlled airway or deeper stability.
- History of difficult sedation experiences (e.g., paradoxical agitation) that increases unpredictability.
In an evidence-minded, safety-first workflow, candidacy is never decided by preference alone. It’s decided by what can be done predictably and safely.
“Are You Awake?” — The Most Accurate Answer
In most medically supervised “awake surgery” settings, you are not “wide awake” in the everyday sense. A more accurate description is: comfortable, monitored, and lightly asleep or deeply relaxed, with local anesthesia doing the heavy lifting for pain control. The goal is a calm, controlled patient experience—without the physiologic depth of full general anesthesia when it isn’t required.
Step-by-Step: How an Awake Breast Lift Is Performed
An awake breast lift follows the same surgical logic as a traditional mastopexy—because the “lift” comes from technique, not from anesthesia. What changes is the anesthesia plan and often the early recovery experience. Below is a clear walkthrough of what typically happens from planning to closure, written for patients who want a true procedural understanding (not a brochure).
Pre-Op Planning and Markings (Why They Matter More Than Most Patients Realize)
Breast lift planning starts before you ever enter the operating room. Markings are usually done while you are standing upright, because gravity affects how the breast sits on the chest. This step helps your surgeon map:
- The intended nipple–areola position and symmetry targets.
- Where skin will be removed (and how much is safe).
- The expected scar pattern based on your incision choice (donut, lollipop, anchor, crescent).
- Where the breast mound should be reshaped to create balanced projection.
This planning phase is also where surgeon and patient align on the “trade-offs”: scar length versus lift power, and upper pole fullness versus “natural” slope.
Local Anesthesia and Twilight Sedation: Comfort Is Layered
In an awake breast lift, comfort is not an afterthought—it is engineered. Most protocols rely on a combination of:
- Local anesthesia to numb the surgical area (so pain signals are blocked at the source).
- Twilight sedation to reduce anxiety, awareness, and time perception.
- Continuous monitoring so the team can fine-tune sedation and maintain stability throughout.
The goal is a calm, controlled experience where you are not “white-knuckling” through surgery. Many patients report feeling sleepy, relaxed, and surprised at how quickly time passes.
Incisions and Access: Matching the Pattern to the Problem
Once the anesthesia plan is working, the surgeon creates the planned incisions. The incision pattern is not simply cosmetic; it dictates how much control the surgeon has to reshape the breast and reposition the nipple–areola complex safely.
- Donut (periareolar): Around the areola; best for mild sagging and limited reshaping needs.
- Lollipop (vertical): Around the areola plus a vertical line to the crease; strong shaping control for many patients.
- Anchor (inverted-T): Adds a crease incision; most control for significant sagging or substantial skin excess.
- Crescent: Limited incision for very modest nipple elevation in highly selected cases.
A key “expert patient” insight: if a minimal-scar pattern cannot safely remove enough excess skin without tension, it can backfire—leading to widened scars, delayed healing, areolar distortion, or a less stable long-term contour.
Reshaping the Breast Mound: The Part That Creates the Lift
A breast lift is not only about removing skin. For long-lasting results, surgeons often reshape internal breast tissue so the new contour is supported from within. Depending on your anatomy and technique, this may involve:
- Redistributing breast tissue to improve projection (a more youthful contour).
- Reducing lower-pole stretch and narrowing a widened breast footprint.
- Creating a more centered breast mound on the chest wall.
This is also where surgeon skill significantly influences whether the result looks “naturally rejuvenated” versus unnaturally tight or flattened.
Nipple–Areola Repositioning and Areola Resizing
One of the defining elements of mastopexy is raising the nipple–areola complex to a more youthful position while preserving blood supply and sensation as much as possible. In many breast lift plans, the areola can also be resized if it has stretched over time.
The critical concept is safety: the nipple is not simply “moved like a sticker.” Instead, it is repositioned while maintaining living tissue connections that preserve vascularity. This is why the degree of lift and the chosen incision pattern matter so much.
Closure Strategy: How Scars Are Influenced (But Not Fully “Controlled”)
Scars are influenced by many variables—skin quality, genetics, tension, aftercare, and incision design. Surgical closure aims to minimize tension and align edges precisely. In many cases, layered closure techniques are used to support the skin and reduce the risk of widened scars.
Even with excellent technique, scar maturation takes time. Most patients see the largest visible improvements in scar appearance over months, not weeks.
Dressings, Surgical Bra, and Discharge Planning
After the final dressings are applied, you’ll typically be placed into a surgical bra (or supportive garment) designed to reduce swelling and protect the new shape. Discharge planning includes guidance on:
- How to sleep (often elevated, avoiding pressure on the breasts).
- How to manage early swelling and discomfort.
- What activity is allowed in the first days.
- Red flags that require immediate medical attention.
In an awake approach, many patients value the potential for a smoother early “come-down” compared with general anesthesia—but your surgical team’s instructions still matter more than how you feel on day one.
Combining Procedures for Better Balance
Many patients don’t want “a lift” in isolation—they want a proportionate, stable shape that fits their body and goals. The smartest surgical plans are often the ones that define what the lift can do on its own (position and shape), then add only what’s needed to achieve the desired volume distribution. The key is avoiding overcorrection: a “more is more” mindset can create unnatural results, increased scar tension, or increased long-term droop.
Breast Lift with Implants: When Upper-Pole Fullness Is a Priority
A breast lift with implants can address both position (lift) and volume (implant). This is typically considered when:
- You want a fuller upper pole that a lift alone cannot predictably create.
- You have significant volume loss after pregnancy or weight changes.
- You want a more “round” or more defined silhouette.
Expert-level planning focuses on balance: choosing an implant size that enhances shape without overloading the skin envelope. Oversizing can increase tension on incisions and increase the risk of a less stable long-term result.
Breast Lift with Fat Transfer: Subtle Volume, Natural Feel
A breast lift with fat transfer is often considered for patients who want modest volume enhancement with a more natural look and feel. In selected cases, fat transfer can help:
- Improve upper-pole softness or mild fullness.
- Correct minor contour irregularities or asymmetry.
- Support a more natural transition zone (especially in leaner patients).
Because fat transfer is not a “guaranteed permanent” volume solution in the same way an implant is, it is best approached as a refinement tool—ideal for patients who value subtlety.
Mommy Makeover Pairing: Strategy Matters More Than the Name
Mommy makeover is a broad term, but the underlying idea is practical: pregnancy and major weight changes often affect multiple areas at once. A common pairing is a breast lift with abdominal contouring. The key is medical planning—operative time, recovery logistics, and staged versus combined procedures must be individualized to maintain safety and optimize healing.
For the expert patient, the right question is not “Can I combine procedures?” but “What combination is safest and most predictable for my anatomy, my goals, and my recovery timeline?”
Awake Breast Lift Recovery Timeline and Aftercare
Breast lift recovery is a process, not a single milestone. Your “day one” comfort can feel surprisingly manageable, but the real goal is controlled healing: protecting incisions, minimizing swelling, supporting tissue blood flow, and preventing avoidable setbacks. In an awake breast lift (local anesthesia + twilight sedation), many expert patients focus on early clarity and reduced post-anesthesia grogginess—but the fundamentals of surgical recovery remain the same: follow your surgeon’s instructions, respect tissue healing timelines, and treat swelling and scar maturation as normal biological phases.
The First 72 Hours: Control Swelling, Protect Incisions, Stay Ahead of Discomfort
The first three days are about stability. Expect tightness, swelling, and tenderness—more “pressure” than sharp pain for many patients. Your priorities are simple and practical:
- Support: Wear the recommended surgical bra/support garment as instructed to protect shape and reduce swelling.
- Positioning: Sleep on your back, slightly elevated, to reduce swelling and avoid pressure on incisions.
- Movement: Gentle walking helps circulation, but avoid lifting, pushing, pulling, or overhead arm movements.
- Hydration and nutrition: Healing is energy-intensive. Prioritize protein and fluids.
- Medication adherence: Take prescribed medications exactly as directed; don’t “tough it out” and fall behind.
Expert-patient note: Many early “complications” start as small rule breaks—lifting a suitcase, sleeping on your side too soon, or returning to a high-heart-rate workout early. Treat the first 72 hours as a surgical protection phase, not a test of toughness.
Week 1: The Protective Phase (Most Restrictions Live Here)
Week 1 is when swelling and bruising often look worse before they look better. Your breasts may sit higher than expected, and symmetry can look “off” temporarily due to uneven swelling—this is usually normal in early healing. Typical priorities include:
- Incision care: Keep incisions clean/dry per your surgeon’s protocol and avoid tension on closure lines.
- Activity limits: No heavy lifting, no gym, no vigorous household chores. Keep arm motion gentle and below shoulder level if instructed.
- Monitoring: Watch for red flags (listed below) and communicate early if something feels “not right.”
Many patients can do desk-level activities within 7–14 days, but that is not the same as being “healed.” Think functional recovery (doing daily tasks) versus biological recovery (tissues regaining strength).
Week 2: Early Normalization (When Patients Feel Better Than They Actually Are)
By week 2, many patients feel a meaningful improvement in comfort and energy. This is also when people are tempted to “return to normal” too quickly. In reality, incisions are still vulnerable to tension and swelling is still evolving. Common expectations:
- Swelling: Usually improving, but still present—especially later in the day.
- Sensation changes: Numbness, tingling, or hypersensitivity can occur and may fluctuate.
- Work: Many return to non-physical work duties if pain is controlled and driving is permitted.
The expert strategy is to keep your activity “under threshold”: do enough movement to support circulation, but not enough to spike swelling and strain incisions.
Weeks 3–6: Gradual Return (Strength Builds Slowly)
This phase is about controlled progression. Swelling continues to settle, tissues soften, and your breast shape begins to look more “you.” Many patients are cleared for increasing activity gradually, often in steps. Typical guidance includes:
- Exercise: Usually reintroduced in a staged way (walking → light lower-body → controlled upper-body later), based on surgeon clearance.
- Support bras: Continued use may be advised to stabilize healing tissues.
- Scar care: If your surgeon approves, scar-management routines often start/continue during this window.
Important: “Pain-free” does not mean “risk-free.” Tissue strength and scar maturation lag behind how good you feel.
Months 3–12: Scar Maturation and Final Shape
The final result of a breast lift is not judged at 2–4 weeks. It’s judged over months. Scars typically fade and soften gradually, and breast shape continues to refine as swelling resolves and tissues settle into their new architecture. Many surgeons consider 6–12 months the true window for assessing scar maturity and stable shape.
Recovery at a Glance: Week-by-Week Table
| Timeframe | What You May Feel | Primary Focus | Common “Don’t Do This” Mistake |
|---|---|---|---|
| Days 1–3 | Tightness, swelling, tenderness | Protect incisions, gentle walking, sleep positioning | Overusing arms / lifting luggage |
| Week 1 | Swelling/bruising fluctuates | Incision care, strict activity limits | Sleeping on side/stomach too soon |
| Week 2 | Energy improves, discomfort drops | Stay under threshold; avoid tension | Returning to full routine too early |
| Weeks 3–6 | Softening, shape looks more natural | Gradual activity return, scar routine (if cleared) | High-intensity workouts before clearance |
| Months 3–12 | Ongoing refinement | Scar maturation, long-term follow-up | Judging final results too early |
Accelerated Recovery & Safety Protocol: HBOT + LLLT (Why Some Clinics Add It)
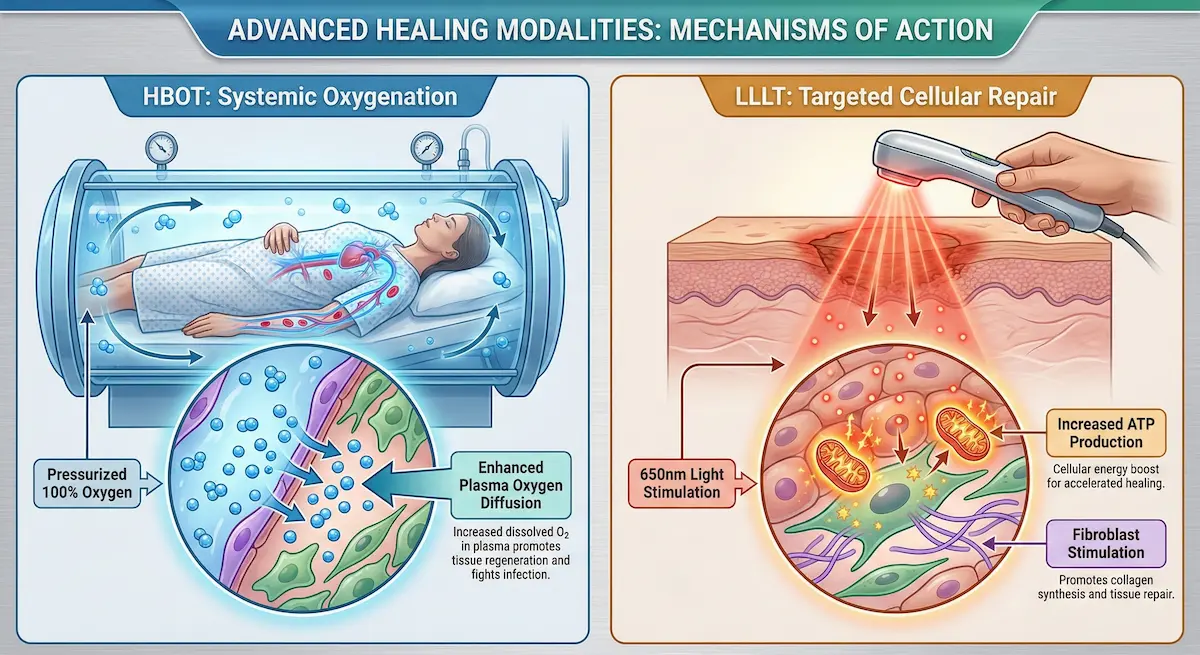
For expert patients, the most compelling recovery strategies are the ones that make biological sense: improve oxygen delivery, reduce inflammation, support collagen remodeling, and lower infection risk. AKM Clinic frames its recovery technologies as a coordinated system—using Hyperbaric Oxygen Therapy (HBOT) for systemic tissue oxygenation and Low-Level Laser Therapy (LLLT) for targeted cellular acceleration. In their materials, HBOT is described as exposing the patient to 100% oxygen in a pressurized environment to enhance oxygen diffusion into healing tissues, supporting regeneration and recovery. LLLT is described as a 650nm “soft laser” approach designed to stimulate cellular activity without heat damage, including ATP (cellular energy) support and fibroblast/collagen stimulation.
- HBOT (systemic “macro” support): Positioned to reduce inflammation, support lymphatic drainage, promote tissue survival/regeneration, enhance scar healing via fibroblast stimulation, and create a hostile environment for certain bacteria while boosting immune response.
- LLLT (targeted “micro” support): Positioned to accelerate cellular repair (ATP), enhance collagen synthesis by stimulating fibroblasts, and serve as an adjunct to further reduce swelling and redness.
AKM Clinic’s own framework describes this as a macro-to-micro sequence: HBOT builds the oxygen-rich foundation, then LLLT supports cellular metabolism and collagen-building within that environment—aiming to reduce “social downtime” and support higher-quality healing.
Red Flags: When to Contact Your Surgeon Immediately
Some symptoms are normal; some require urgent evaluation. Contact your surgical team promptly if you experience:
- Sudden, rapidly increasing swelling (especially on one side) or severe pressure not relieved by medication.
- Fever or chills, or worsening redness/warmth spreading around incisions.
- Drainage that is foul-smelling, thick, or increasing rather than decreasing.
- Shortness of breath, chest pain, or calf swelling/pain (medical emergency symptoms).
- Darkening skin around the nipple–areola complex or incision edges (needs urgent assessment).
Expert-patient principle: early communication is not “overreacting.” It’s how small issues stay small.
Continuity of Care: Virtual Follow-Up Milestones
Long-term outcomes depend on long-term oversight. A structured follow-up schedule helps monitor scar maturation, swelling resolution, and symmetry refinement. AKM Clinic describes scheduled virtual follow-ups at 1, 3, 6, and 12 months as part of its continuity-of-care model, which is particularly relevant for international patients returning home.
Scars, Scar Care, and “One-Year” Expectations
Scars are one of the biggest decision drivers for breast lift patients—and also one of the most misunderstood parts of recovery. The most important expert-patient reality is this: scars are not “created” only by the incision pattern. They are shaped by tension, blood supply, skin quality, your genetics, and how consistently you protect healing tissues in the first weeks. A thoughtful surgical plan chooses an incision that allows the surgeon to lift and reshape the breast with low tension, because low tension is one of the strongest levers for better-looking scars over time.
Where Scars Typically Sit (By Incision Type)
Breast lift scars are predictable in location but variable in how they mature. Where you will typically see scars depends on the incision pattern:
- Donut (periareolar): A scar at the border of the areola (often camouflaged by the natural color transition).
- Lollipop (vertical): A periareolar scar plus a vertical scar down to the breast crease.
- Anchor (inverted-T): A periareolar scar, a vertical scar, and a scar along the inframammary fold (breast crease).
- Crescent: A small scar along the upper areolar border (limited use, highly selected cases).
For many patients, the “most visible” portion early on is the vertical line. Over time, the crease scar (anchor) is often hidden by natural breast position, while the areolar scar can blend into the pigmented border.
Scar Maturation Timeline: What’s Normal vs. What’s Not
Scar healing happens in phases. Knowing the timeline can prevent unnecessary anxiety:
- Weeks 0–6: Incisions look fresh. Redness and firmness are normal. The priority is keeping tension low and preventing irritation.
- Months 2–6: Scars can look more red before they look better. This is a common “scar panic” window.
- Months 6–12: Many scars flatten, soften, and fade. This is where “one-year expectations” usually become clearer.
Not every scar fades to near-invisible—some patients are prone to thickened or raised scars. The goal is to stack the odds in your favor through surgical planning (low tension, good blood supply) and disciplined aftercare.
Scar Care Protocol (Evidence-Informed Principles)
Your surgeon’s instructions come first, but these are commonly used principles once incisions are fully closed and your surgeon clears you:
- Silicone support: Silicone sheets or gel are often used to support scar hydration and reduce thickening.
- Sun protection: UV exposure can darken scars. Treat scars like “new skin” that needs protection for months.
- Friction control: Avoid aggressive rubbing, tight underwires too early, or irritation from clothing seams.
- Massage (only when cleared): In some cases, guided scar massage may help softening—but timing matters.
- Consistency: Scar care is a long game. The difference is often adherence over months, not intensity for a week.
Breast Lift Scars After One Year: What Patients Can Realistically Expect
At the one-year mark, many patients see scars that are flatter, lighter, and less noticeable than in early months—especially if tension was controlled and aftercare was consistent. However, realistic expectations matter:
- Most likely: A visible but “fine-line” scar that blends better with skin tone over time.
- Possible: Areas of redness that persist longer (often improves with time, sometimes needs targeted scar therapy).
- Less common but important: Hypertrophic scarring (raised) or wider scars—more likely when tension, irritation, or healing issues occurred early.
If scars remain prominent, there are escalation options (from medical-grade scar management to targeted treatments). The best next step is surgeon-guided evaluation—because “treating the wrong scar problem” wastes time and can irritate healing skin.
Risks, Complications, and How to Reduce Them
No ethical medical guide minimizes risk. A breast lift is a real surgical procedure with real trade-offs: you are exchanging scars for a lifted shape and improved nipple position. The “awake” anesthesia approach can improve certain aspects of the experience for selected patients, but it does not remove surgical risk. What matters most is proper candidacy screening, a sterile environment, experienced surgical judgment, and disciplined recovery behavior.
Early Risks (Bleeding, Infection, Wound Healing Issues)
Early complications tend to occur in the first days to weeks. The most important include:
- Bleeding/hematoma: A collection of blood that can cause rapid swelling, pressure, and asymmetry. It may require urgent evaluation.
- Infection: Typically presents with increasing redness, warmth, pain, fever, or abnormal drainage. Early treatment matters.
- Delayed wound healing: Small wound openings can happen, especially where tension is highest (often at junction points in anchor patterns).
Risk reduction is a system: candidacy screening (including nicotine cessation), meticulous technique, and reliable monitoring protocols during and after surgery.
Aesthetic Risks (Asymmetry, Bottoming Out, Recurrent Ptosis)
Even with excellent surgery, the breast is dynamic tissue. Aesthetic risks can include:
- Asymmetry: Some degree of natural asymmetry exists pre-op; swelling can exaggerate it early. True asymmetry is evaluated later.
- Bottoming out: A situation where the lower pole stretches and the nipple appears higher relative to the breast mound over time.
- Recurrent ptosis: Skin and tissue can stretch again due to aging, gravity, pregnancy, or weight changes.
Surgeons reduce these risks by matching incision choice to ptosis severity, reshaping internal tissue for support, and avoiding overloading the skin envelope (especially in lift-plus-implant plans).
Sensation, Nipple Blood Supply, and Breastfeeding Considerations
Because mastopexy involves reshaping tissue and repositioning the nipple–areola complex, sensory changes can occur. Patients may experience temporary numbness, tingling, or hypersensitivity. In many cases, sensation improves over time, but it can be prolonged or, less commonly, persistent.
Blood supply to the nipple–areola complex is a critical safety focus in any breast lift. Risk increases with more extensive lifts, complex revisions, smoking/nicotine exposure, and certain anatomy. This is one reason strict candidacy screening and clear pre-op instructions are not “optional.”
Breastfeeding after a lift is possible for some patients, but it cannot be guaranteed. If future breastfeeding is a major priority, that should be discussed early, because it can influence both timing and technique selection.
Revision Surgery: Why It Happens and What It Usually Fixes
Revision does not always mean a “failed” surgery; sometimes it reflects biology, healing variability, or evolving goals. Common revision drivers include:
- Persistent asymmetry after full healing
- Scar concerns (widening, thickening)
- Shape refinement (minor contour issues)
- Recurrent ptosis over time
The expert-patient mindset is to evaluate results on the correct timeline. Final shape and scar maturity are judged over months, not weeks—so decisions about revision should be made with a long-term view and a surgeon-led assessment.
Awake Breast Lift Results: Natural Rejuvenation, Not Alteration
Most patients considering a breast lift are not trying to “change” their body. They want to restore what time, gravity, pregnancy, or weight changes have altered—without creating an obvious, overcorrected, or “operated” look. A high-quality breast lift respects proportion: it restores nipple position, improves the breast footprint on the chest, and reshapes the mound with stability in mind.
What a “Natural” Breast Lift Looks Like
A natural-looking lift typically has:
- Balanced upper-to-lower pole shape (not overly round or unnaturally high).
- Nipple position that looks anatomically believable and symmetrical.
- Low-tension scars that mature predictably over time (because the plan matched the ptosis severity).
- Shape that fits your frame rather than chasing a one-style aesthetic.
This “natural-first” principle is often summarized in a simple idea: the best aesthetic surgery is the kind that looks like you—just restored. AKM Clinic describes this philosophy as “Rejuvenation, Not Alteration” and frames it as a guiding standard across procedures.
The Trade-Off Triangle: Shape vs. Scar vs. Longevity
Every breast lift plan sits inside a trade-off triangle:
- Shape: How much reshaping and projection you want.
- Scar footprint: How much incision access is required to safely create that shape.
- Longevity: How stable the result is as the tissue settles and ages over time.
Trying to maximize all three can create conflict. For example, insisting on the smallest scar pattern despite moderate-to-severe ptosis can increase tension and reduce longevity. Conversely, choosing an incision pattern with adequate control can lower tension and improve predictability—even if the scar footprint is larger on day one.
Surgeon’s Insight: “The most successful aesthetic surgery is one that goes unnoticed.”
Awake Breast Lift Cost Analysis: NYC / Los Angeles vs. Istanbul
Cost is not just a price tag—it’s a reflection of geography, operating overhead, facility fees, anesthesia type, and the complexity of your surgical plan. Expert patients tend to compare against premium U.S. metros (like New York City or Los Angeles) for a reason: those markets are often a “top of range” benchmark. The smarter question isn’t “Where is it cheapest?” but “Where can I get predictable, high-standard care with transparent pricing and safety infrastructure?”
What Drives Breast Lift Cost in Premium U.S. Markets
In the U.S., you’ll typically see cost influenced by:
- Surgeon fee (experience, demand, and region)
- Anesthesia fees (type of anesthesia + anesthesia provider)
- Facility/operating room fees (surgery center vs. hospital setting)
- Complexity factors (degree of ptosis, revision status, combined procedures like implants or fat transfer)
- Geographic overhead (rent, staffing costs, insurance, and cost of living)
For context, the American Society of Plastic Surgeons (ASPS) notes an average surgeon/physician fee for mastopexy, but also clearly cautions that this figure does not include anesthesia or facility costs, which can add significantly to the total.
Reality Check: Typical NYC and LA Benchmarks (Patient-Reported)
Because pricing varies widely by provider and facility, patient-reported benchmarks can help frame the range. RealSelf’s “costs in major U.S. metros” list shows average figures of $14,130 for New York City and $13,636 for Los Angeles for breast lift procedures (patient-reported averages).
| Location / Reference Point | What the Number Represents | Example Benchmark | Important Caveat |
|---|---|---|---|
| ASPS (U.S. average) | Average surgeon/physician fee | $6,816 | Does NOT include anesthesia/facility/other fees |
| New York City (major metro) | Patient-reported average total | $14,130 | Varies by provider, complexity, and facility |
| Los Angeles (major metro) | Patient-reported average total | $13,636 | Varies by provider, complexity, and facility |
Why Turkey Can Be Lower Cost Without “Lower Standards”
A key concern for U.S. patients is whether a lower price implies lower safety. AKM Clinic’s own materials directly address the cost gap as a macroeconomic reality—not a quality compromise—citing the USD-to-TRY exchange rate and lower national operational costs (such as staffing and rent) as primary drivers.
Importantly, their value proposition is positioned around maintaining “world-class” inputs and standards—such as using FDA-approved materials and operating in JCI-accredited hospitals—while benefiting from lower baseline operating costs.
What an All-Inclusive Model Typically Covers (Transparency Matters)
For international patients, a major hidden-cost risk is “fee stacking”—paying separately for transfers, garments, medications, testing, and aftercare. AKM Clinic describes an all-inclusive structure that can include items such as:
- Your surgical procedure
- Anesthesia and operating room fees
- Pre-operative tests
- 5-star hotel accommodation
- VIP airport and clinic transfers
- Post-op medications and garments
- Long-term virtual follow-up care
This framework is presented as a trust mechanism: reducing uncertainty so the patient can focus on preparation and recovery.
Choosing the Right Surgeon and Facility (Safety Checklist)
The fastest way to reduce risk in breast lift surgery is to choose the right environment and the right team. Expert patients tend to look beyond marketing and focus on systems: screening, sterility, monitoring, and credentials that hold up under scrutiny. Use the checklist below to evaluate any provider—anywhere in the world.
Credentials That Actually Matter
- Board certification in the surgeon’s specialty
- Procedure-specific experience (not just “breast surgery” broadly)
- Revision competence (ability to handle complexity if anatomy is challenging)
- Clear complication plan (what happens if there is bleeding, infection, delayed healing)
AKM Clinic’s materials also reference that many top Turkish surgeons hold European Board certifications (e.g., EBOPRAS) and position these credentials as comparable to U.S. board rigor.
Facility Standards: Don’t Treat This as a “Nice-to-Have”
Ask where your surgery is performed and what standards are followed. AKM Clinic frames safety as “non-negotiable,” referencing elements such as rigorous sterilization standards, continuous vitals monitoring during procedures, and strict pre-operative screening for candidacy.
Awake/Twilight Sedation Questions to Ask (Any Clinic)
- Who is monitoring you during the procedure, and what vitals are tracked continuously?
- What is the escalation plan if you become uncomfortable or medically unstable?
- How is nausea, anxiety, or pain managed during and after surgery?
- What pre-op screening is required to confirm you’re a suitable candidate?
The Medical Journey for International Patients (A Practical, Safety-First Workflow)
For patients traveling internationally, the biggest risk is rarely the flight itself—it’s poor coordination: rushed timelines, unclear pre-op screening, inconsistent aftercare, and weak follow-up. A well-run international workflow should feel like a medical pathway, not a tourism itinerary. The goal is to reduce uncertainty, control variables, and keep decision-making clinical and transparent from the first consult to the final scar check.
Step 1: Virtual Consultation and Pre-Op Screening (Where Safety Starts)
A legitimate surgical journey begins with candidacy—not pricing. A structured consultation should include:
- Goal clarification: lift alone vs. lift + implants vs. lift + fat transfer.
- Technique planning: donut vs lollipop vs anchor based on ptosis and skin quality.
- Anesthesia fit: whether local anesthesia + twilight sedation is appropriate for your medical profile and comfort level.
- Risk profiling: nicotine use, prior surgeries, bleeding/clotting history, and recovery logistics.
For the expert patient, this is also where you should ask for a clearly written plan: what incision is recommended, why it’s recommended, and what trade-offs you are accepting (scar footprint vs lift power vs long-term stability).
Step 2: Arrival, Logistics, and Timing (Minimizing “Rushed Medicine”)
International surgery should be scheduled to allow a calm buffer—not a tight rush from landing to operating room. A patient-centered schedule usually includes:
- Arrival buffer: time to rest, hydrate, and reduce travel-related stress.
- In-person assessment: physical exam and confirmation of the surgical plan.
- Pre-op testing: medical clearance and baseline vitals/labs where appropriate.
Clinics that run an all-inclusive model often include coordinated transfers and accommodation to reduce friction points that can derail preparation and recovery.
Step 3: Procedure Day Flow (What a “Calm, Controlled” Experience Looks Like)
On procedure day, the most important markers of quality are not décor or marketing—they are process controls. In an awake breast lift, the “good” version of the day includes:
- Clear consent and re-confirmation: incision plan, goals, and expectations reviewed one last time.
- Monitored sedation: comfort is adjusted in real time; safety monitoring remains continuous.
- Low-tension technique focus: internal shaping and tension management to improve scar predictability.
- Discharge planning: written instructions, medication schedule, and emergency contact protocol.
Expert-patient tip: Ask how the team handles “what if” scenarios—nausea, anxiety spikes, unexpected bleeding, or discomfort—because the presence of a plan is a strong signal of competence.
Step 4: Early Post-Op Checks in Istanbul (Before You Fly Home)
International patients should not fly home without a proper early assessment. A responsible pathway typically includes:
- Incision review: checking closure integrity and early wound healing.
- Swelling and symmetry baseline: setting realistic expectations for the coming weeks.
- Garment guidance: confirming bra/support strategy and what to avoid (underwire too early, friction points).
- Fitness-to-fly guidance: individualized clearance and comfort recommendations.
Step 5: Long-Term Virtual Follow-Up (Where Many Clinics Fail—and Outcomes Suffer)
Scar maturation and shape refinement happen over months, not days. For international patients, structured virtual follow-ups are not “nice to have”—they are continuity of care. A robust follow-up timeline commonly includes check-ins at:
- 1 month: incision stability, swelling pattern, early scar strategy.
- 3 months: shape settling, activity normalization, scar progression.
- 6 months: maturity checkpoint for scars and symmetry.
- 12 months: long-term outcome assessment and any refinement discussion.
FAQ: Questions About Awake Breast Lift
These are the questions expert patients ask most often when researching an awake breast lift. The answers are intentionally direct, clinically grounded, and designed to clarify decisions—not oversimplify them.
Are you awake during a breast lift under local anesthesia?
In most “awake” breast lift protocols, you are not fully alert in the everyday sense. You are typically deeply relaxed or lightly asleep with local anesthesia blocking pain and twilight sedation reducing awareness and anxiety. Many patients have limited memory of the procedure.
What does twilight sedation feel like?
Most patients describe twilight sedation as a calm, drowsy state where time feels shorter. You may drift in and out of light sleep, feel minimal anxiety, and remain comfortable. The key point: sedation is adjustable and should be monitored continuously.
Is twilight sedation safer than general anesthesia?
“Safer” depends on your medical profile and the complexity of surgery. For selected patients, avoiding full general anesthesia can reduce certain downsides (like deeper postoperative grogginess or nausea). However, the safest approach is the one matched to your health status and surgical scope, with proper monitoring and a clear escalation plan.
How long is breast lift recovery week by week?
Most patients experience the strictest restrictions in the first 1–2 weeks. Weeks 3–6 are typically gradual normalization. Scar and shape refinement continues for months, with many surgeons judging “final” scar maturity and stable shape in the 6–12 month range.
What are the disadvantages of a breast lift?
The main trade-offs are:
- Scars: you exchange sagging correction for incision lines that take months to mature.
- Healing variability: swelling, scar quality, and symmetry can vary early on.
- Longevity limits: aging, gravity, pregnancy, and weight changes can gradually stretch tissue again.
- Potential sensation changes: often temporary, occasionally prolonged.
What incision type will I need (lollipop vs anchor vs donut)?
It’s determined by your ptosis severity, skin quality, and reshaping needs. Mild sagging may fit a donut lift. Many patients fall into the lollipop/vertical category. Significant ptosis or major skin excess often requires an anchor pattern for safe, low-tension control.
Can I combine a breast lift with implants?
Yes—especially if upper-pole fullness is a primary goal. The critical expert-patient point is sizing discipline: oversizing can increase tension on scars and reduce long-term stability. The best plan balances shape goals with tissue limits.
Can I combine a breast lift with fat transfer?
Yes, in selected cases. Fat transfer is often used for subtle volume and contour refinement with a natural look and feel. It should be approached as a shaping tool, not a guaranteed large-volume augmentation.
When can I return to work and exercise?
Many patients can return to desk-based work within 1–2 weeks, depending on comfort and surgeon clearance. Exercise is typically reintroduced gradually—often with walking first and more intense training later—because tissue strength builds slower than your energy returns.
What will my scars look like after one year?
Many patients see scars that are flatter, softer, and lighter by the one-year point. The biggest factors are low tension, good blood supply, consistent scar care, and avoiding early irritation. Some patients are predisposed to thicker scars, which may require targeted scar management.